Predictors of time to viral load suppression in young people in Gwanda District, Zimbabwe, 2021
Mutizwa Thomas Mupedziswa1, Rudo Chikodzore2, Gerald Shambira1, Mujinga Karakadzai1, Notion Tafara Gombe3,4, Mufuta Tshimanga1,2,3,4
1University of Zimbabwe, Department of Primary Health Care Sciences: Family Medicine, Global and Public Health Unit, Harare, Zimbabwe, 2Matabeleland South Provincial Medical Directorate, Ministry of Health and Child Care, Bulawayo, Zimbabwe, 3African Field Epidemiology Network, Harare, Zimbabwe, 4Zimbabwe Field Epidemiology Training Program, Harare, Zimbabwe
&Corresponding author
Mutizwa Thomas Mupedziswa, University of Zimbabwe, Department of Primary Health Care Sciences: Family Medicine, Global and Public Health Unit, Harare, Zimbabwe.
Introduction:
Antiretroviral Treatment (ART) aims to achieve and maintain viral suppression in HIV patients. Unsuppressed viral load leads to HIV transmission, susceptibility to infections, and premature death. Gwanda District failed to meet the 90% national viral load suppression target. Predictors of time to viral load suppression in ART-initiated young people were determined to generate information to improve the provision of HIV treatment in Gwanda District.
Methods:
Complete records of young people initiated on ART in Gwanda District were reviewed. Data was captured using Microsoft Excel and analyzed using Epi info 7. Kaplan Meier log-rank test was used to compare time to event experience between groups and cox proportional hazard model to determine significant predictors.
Results:
Median time to suppression was 207 days and (interquartile range [IQR] 204-215). Most were females 502/667 (75.4%) and majority age group was 21-25 years (64.3%). Categories of Cotrimoxazole preventative therapy (CPT), baseline CD4, baseline viral load, and Tuberculosis Preventative therapy (TPT) showed significant curves differences (P-value<0.00). Independent predictors of time to suppression included baseline CD4 count [Adjusted Hazard Ratio (AHR) =2.52, 95% CI: 1.94-3.28], CPT (AHR=3.18, 95% CI: 2.31-4.38), TPT (AHR=5.48, 95% CI: 4.22-7.11), substance use (AHR=1.56, 95% CI: 1.14-2.14), and migration (AHR=1.549, 95% CI: 1.25-1.92).
Conclusion:
Predictors of time to suppression were baseline CD4, baseline viral load, migration and substance use probably due to defaulting by substance users and reduced ART access among migrants. Preventative therapy initiation reduced time to suppression. We recommended intensified follow-up, improved access to HIV services among migrants and facilitation of HIV continuum of care cross border coordination.
Introduction

HIV is estimated to have claimed the lives of 36.5 million individuals worldwide [1]. In 2020 it was estimated that over 37.7 million people were living with HIV, two-thirds of whom (25.4 million) were in the WHO African Region [1-3]. Globally, an estimated 1.8 million young people between the ages of 15-25 are HIV infected with the majority (89%) residing in sub-Saharan Africa [2,3]. An estimated 20,000 young people aged 15-25 years in Zimbabwe are estimated to be living with HIV [4]. While the global mortality from HIV/AIDS in adults has declined by 51% and HIV incidence has declined by 45% since its peak a decade ago, AIDS-related deaths and the HIV incidence among young people aged 15-25 years remains high with the world still behind on achieving the targets set for young people [2,3,5]. In sub-Saharan Africa, girls represent six out of seven new HIV infections among adolescents aged 15-19 years [3,6]. Young women aged 15-25 years are twice as likely to be living with HIV than men [3,6]. In 2014 the UNAIDS and member states came up with objectives aimed at terminating the HIV/AIDS pandemic by 2030 [3]. The objectives state that 90% of persons living with HIV should recognize and know their status, 90% of those who have known their status are placed in management, and 90% of those in management are virally suppressed which is having an HIV viral load of less than 1000 copies/ml of blood [3-5,7].
Zimbabwe remains one of the countries with the highest HIV prevalence in sub-Saharan Africa at 12.8%, with 1.4 million people living with HIV in 2019 [
4,
8]. In 2020, 86.8% of the people living with HIV in the country were aware of their status and 97% of those diagnosed were on treatment. Of the people diagnosed and on treatment, 90% were virally suppressed [
4]. HIV viral load suppression in young people 15-25 years in Gwanda District failed to meet the average national viral load suppression of 90% despite the efforts by partners through community adolescent treatment supporters in the district which aim to improve adherence, psychosocial well-being, linkage, and retention in the care of the young people 15-25years old. Viral load suppression in people living with HIV is both a global and national objective as set out by the Joint United Nations Programme on HIV and AIDS [
1,
3]. Reduction of morbidity and mortality due to HIV and HIV comorbidities involves the prevention of HIV transmission and treatment of people living with HIV. An unsuppressed viral load leads to HIV transmission and susceptibility of HIV patients to opportunistic infections leading to premature death. We investigated the predictors of time to viral load suppression to generate information that assists to improve HIV quality of care and HIV outcomes of persons on ART.
Methods

Study Design and Setting
We conducted a cross-sectional study involving retrospective record review of routinely collected data of people living with HIV in HIV opportunistic infection registers in Gwanda District of Zimbabwe. HIV opportunistic infection registers are registers which contain information about all HIV patients. Gwanda District, located in Matabeleland South Province with a total population of 167,148 has the highest HIV prevalence (17.9%) in Zimbabwe [
4]. The district borders South Africa, and the main economic activities include both formal and informal mining, livestock rearing, and cross-border trading.
Study Population and Sampling
Complete records of HIV patients initiated on ART in 2021 were extracted from opportunistic infection registers in Gwanda District health facilities and reviewed for this study.
Sample size
A sample size of 359 was calculated using the Dobson formula at 95% confidence level with 80% power, using a prevalence of participants with viral load less than 200 cell/ml of 37.3% based on a previous study [
9].
Sampling Frame
All health facilities in Gwanda District offering HIV treatment services were selected. All patient records for the year 2021 were reviewed using a checklist, incomplete records were excluded and complete ones were included in the study. The sampling frame was all records/entries of HIV patients enrolled on ART in the laboratory information management system (LIMS) in all the Gwanda District health facilities for the period of January to December 2021.
Figure 1 shows a schematic diagram of how data were extracted.
Figure 1: Schematic presentation of data extraction of predictors of viral load suppression in young people years in Gwanda District 2021.
Data Capture
Variables that were found to be predictors of time to viral load suppression from the literature include age, sex, employment status, marital status, baseline CD4 count, baseline viral load, tuberculosis infection, tuberculosis preventative therapy (TPT), and cotrimoxazole preventative therapy (CPT) were collected using a data capture tool developed in Microsoft Excel.
Data analysis
Data were analyzed using Epi info™ version 7.2.4, (CDC 2019) to generate frequencies and proportions of the demographic predictors of time to HIV suppression. In addition, medians and interquartile ranges were generated for all variables. Kaplan-Meier survival curve was used to compare the time to viral load suppression between groups; groups that were analyzed included: individuals initiated on CPT compared to those who were not, those initiated on TPT compared to those who were not, and CD4 count at baseline (CD4 >350 vs CD4 <350). Bivariate Cox proportional hazard model analysis was performed for each independent variable to identify statistically significant predictors of time to viral load suppression (p value <0.25). Statistically significant variables (p-value <0.25) were included in the multivariable cox proportional hazard analysis model, p-value <0.05 was used to determine whether or not the variable was significant.
Ethical Considerations
The study was reviewed and approved by the Matabeleland South Provincial Medical Directorate (MS/IEC/04/2022). The data collecting tools had no patient identifiers, unique identifiers were used to maintain anonymity. All the data collected in this study was kept confidential, and only the study investigators had access to individual patient information. Permission to carry out the study was obtained from the Matabeleland South Provincial Medical Directorate, Gwanda District Medical Officer, and from the Health Studies Offices within the Ministry of Health and Child Care.
Results
Demographic Characteristics of HIV-infected people (15-25) years in Gwanda District
The majority of the reviewed records were of female patients 502/667 (75.4) and the majority age group was 21-25 years 428/667 (64.3%).
The median time to viral load suppression in individuals who achieved suppression was 207 days (interquartile range (IQR) 204-215).
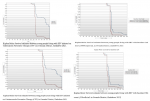
The Kaplan Meier (KM) survival curve shows that there were differences in time to viral load suppression among groups of baseline CD4 count, baseline viral load, CPT, and TPT. The KM curve to compare individuals initiated on Cotrimoxazole Preventative Therapy, on their baseline CD4, their baseline viral load, baseline viral load below 10,000 copies/mL and individuals who did not initiate Tuberculosis Preventative Therapy shows the significant difference in time to viral load suppressions (log-rank p-value <0.001).
The KM curve comparing individuals initiated on Cotrimoxazole Preventative Therapy with those not initiated shows a significant difference in time to viral load suppressions (log-rank p-value <0.001). The median time to HIV suppression in patients initiated on CPT was 221 days´ vs 241 days (20 days´ difference) among patients not initiated on CPT (
Figure 2).
The KM curve to compare individuals based on their baseline viral load shows a significant difference in time to viral load suppressions (log-rank p-value <0.001). Patients with baseline viral load below or equal to 10,000 copies/mL reached suppression within a median of 210 days while patients who had baseline viral load of above 10,000 copies/mL reached suppression in 225 days (15 days´ difference) as shown in
Figure 2.
The KM curve to compare individuals on the basis of their TPT initiation shows a significant difference in time to viral load suppressions (log-rank p-value<0.001). The median time to HIV suppression among patients initiated on TPT was 210 days compared to the median time of 285 days (75 days´ difference) in patients not initiated on TPT as shown in shown in
Figure 2.
The KM curve comparing individuals based on their baseline CD4 also shows a significant difference in time to viral load suppressions (log-rank p-value<0.001). Patients with a baseline CD4 count above 350cells/ml reached suppression earlier with a median time of 200 days than patients who had a baseline CD4 count below 350 cells/ml who had a median time of 220 days (20 days´ difference) as shown in
Figure 2.
Demographic predictors of time to viral load suppression
An analysis of demographic predictors of time to viral load suppression is shown in
Table 1. A bivariate analysis of demographic predictors of time to viral load suppression to obtain Hazard Ratios (HR) showed that there was no statistically significant difference in time prediction by the demographic characteristics of the participants. The young patients (15-20 years), never married, employed, and non-migrants attained viral load suppression earlier compared to their counterparts. While substance users, males and those residing in rural areas achieved viral load suppression later than the females and urban residents.
Table 1 - Non- migrant individuals achieved viral suppression earlier compared to the migrant individuals though this was not significant (HR=1.22, 95% CI: 0.999; 1.505).
Clinical predictors of time to viral load suppression
At bivariate analysis, all the assessed clinical predictors were statistically significantly associated with time to viral load suppression. Individuals who had baseline CD4 count ≥350cell/mL achieved viral suppression earlier than individuals with baseline CD4 <350cell/mL (cHR=1.85, 95% CI: 1.452-2.364). Patients with higher baseline viral load (≥10,000 copies/mL) experienced viral load suppression later than those with low baseline viral load (<10,000 copies/mL) (cHR= 0.377, 95% CI: 0.305- 0.465). Patients who did not have TB at baseline attained viral load suppression earlier compared to those who had TB at baseline (cHR=3.743, 95%CI:2.668-5.250). Patients who did not have other opportunistic infections at baseline attained viral load suppression earlier than those who did not have opportunistic infections at baseline (cHR=3.751, 95%CI: 2.678-5.260). Patients who were on CPT and TPT were more likely to suppress viral load earlier than those patients not initiated on CPT and TPT (cHR=3.63, 95% CI: 2.890- 4.550) and (HR=3.062, 95% CI: 2.247- 4.175) respectively as shown in
Table 1.
Independent predictors of time to viral load suppression
Multivariable analysis, used all the covariates with p<0.25 to determine independent predictors of time to viral load suppression. Baseline CD4 count, Cotrimoxazole prophylaxis, and TPT were statistically significant as shown in
Table 2.
Individuals with baseline CD4 count >350cell/mL were significantly more likely to achieve viral suppression earlier compared individuals with baseline CD4 <350cell/mL (AHR = 2.52, (95% CI 1.94-3.28)). Patients initiated on CPT and TPT were significantly more likely to suppress viral load earlier than patients not initiated on CPT and TPT (AHR = 3.183, (95% CI 2.31-4.38)) and (AHR = 5.478, (95% CI 4.22- 7.11)) respectively. Individuals staying outside the country were more likely to achieve viral suppression earlier compared to those who were living outside the country (AHR = 1.549 (95% CI: 1.252-1.916)).
Discussion
The median time to viral load suppression was 207 days. Moreover, baseline CD4 count, baseline viral load, Cotrimoxazole Preventive Therapy, Tuberculosis Preventive Therapy, and adherence level were identified as the independent predictors of time to HIV viral load suppression.
The study also found that CD4 count at initiation of ART significantly affects the time to viral load suppression among study participants. The time needed for viral load suppression of those who have greater than 350 cells/mm3 CD4 count was less than among those with <350cells/ mm
3 CD4 count. Patients with a CD4 count >350 were two times more likely to have earlier viral suppression. This could be because higher CD4 counts correlate with low viral loads and therefore with a shorter time to suppression. Furthermore, CD4 count has an inverse relationship to viral replication because as the patient's immune status declines, viral replication increases [
8-10]. Low CD4 count may be due to late hospital presentation due to poor health seeking behaviour in young population[
11]. Poor health seeking behaviour in young people is probably due to fear, stigma and mistrust of the health system [
12-14].
This study identified that patients who did not have TB and opportunistic infection at baseline achieved viral load suppression earlier that those who has TB and opportunistic infection at baseline. This finding is consistent to findings from studies conducted in Ethiopia by Mosisa et al 2024 and Bisetegn et al 2021 [
15,
16]. This is probably because opportunistic infections and TB are usually as a result of a weakened immune system, the viral replication increase as the immune system weakens so much so patients with weak immune systems have higher HIV replication rate compared to patients with strong immune systems.
We identified that baseline viral load predicts time to viral load suppression. Patients with higher baseline viral load (≥10,000 copies/mL) experienced viral load suppression later than those with low baseline viral load (10,000 copies/mL). This is could be due to that low plasma viral load means low HIV reservoirs; therefore it takes less time to achieve viral load suppression [
10].
In this study non-migrant patients achieved viral suppression earlier compared to migrant patients. This may be probably because patients living outside the country fail to consistently visit the clinic due to long distances and costs of travel leading which to defaulting due to inconsistent drug supply, and lack of access to HIV treatment and care. Significant number of young people lack the financial resources to pay for services due to unemployment and poverty induced financial instability. A study in Harare by Nyika et al 2016 and Letta in Ethiopia 2015 showed that having an income is a protective factor for late hospital presentation [
14,
17]. In this study substance abusers had delayed viral load suppression compared to non-substance users. Substance users are more likely to have mental health issues which affect ability to make right decisions which impacts drug adherence. Substance abuse in rampant in young people due to age group associated social pressures, unemployment, peer pressure and poverty. Patients with good adherence to ART drugs are more likely to have viral load suppression as compared to those who have poor adherence to ART drugs. This is because ART reduces the multiplication of HIV particles. These finding are similar to findings from studies in Uganda and Zimbabwe [
18,
19].
In this study, Cotrimoxazole Preventive Therapy and Tuberculosis Preventive Therapy reduced the time taken for patients to achieve viral load suppression. Patients who were on CPT and IPT were more likely to suppress the viral load earlier than those patients not initiated on CPT and TPT. Cotrimoxazole prophylaxis has a significant reduction in bacterial infections and mortality. Given the high underlying risk of high viral replication and bacterial infection during the early period, this improvement in co-morbidity could correspond to early viral load suppression. Similarly providing TPT, in turn, reduces the co-infection of TB which further reduce the duration of the viral load suppression since TB is highly associated with the depletion of CD4 T-cell count and high viral load [
9].
Limitations
The major limitation was the inability to evaluate the quality of HIV treatment and care services in the district since the study was a secondary data analysis.
Conclusion
We identified that a low baseline viral load, higher level of baseline CD4 count, exposure to preventive therapies such as Cotrimoxazole and Isoniazid prophylaxes significantly reduce the time to viral load suppression among young people 15-25 years of age living with HIV. In addition, substance abusers and people who were on treatment but were living outside the country had an increased time to viral suppression than those living in the country.
Recommendations
We recommended that stakeholders working on the HIV program can maintain and potentially improve the time to viral load suppression by improving access to targeted viral load testing and CD4 count, and continuous monitoring for all patients on ART, starting from the first day of treatment. In addition, we recommended health education in young people to improve health seeking behaviour in young people, early health seeking behaviour and early HIV testing which leads to early treatment. Furthermore, we recommended healthcare professionals and adherent supporters who offer HIV services follow up with HIV patients and intensify adherence support for those patients with poor adherence and substance abusers. As a long-term recommendation, the National Aids/ TB program should facilitate cross-border coordination on the HIV continuum of care so that individuals living outside the country can easily access health care in the areas they live.
What is known about this topic
- The time to HIV viral load suppression is depends on the individual`s adherence to ART treatment
What this study adds
- This study adds new information that delays in HIV viral load suppression may be due non-adherence in individual accessing health care in countries that they do not live in.
- Substance abuse prolongs the time taken to achieve viral load suppression.
Competing interests
The authors declare no competing interest.
Funding declaration
The Ministry of Health and Child Care, the University of Zimbabwe, Department of Primary. Health Care Sciences: Family Medicine, Global and Public Health Unit supported with material resources in coming with this manuscript.
Authors' contributions
Mutizwa Thomas Mupedziswa: roles conceptualization, formal analysis, resources, writing (original draft), writing (review & editing). Rudo Chikodzore: roles conceptualization, formal analysis, supervision, writing (original draft). Gerald Shambira: roles conceptualization, formal analysis, supervision, writing (original draft), writing (review & editing). Mujinga Karakadzai: roles conceptualization, formal analysis, supervision, writing (original draft), writing (review & editing). Notion Tafara Gombe: roles conceptualization, formal analysis, methodology, writing – original draft, writing: review & editing. Mufuta Tshimanga: roles conceptualization, formal analysis, methodology, supervision, validation, writing (original draft), writing (review & editing).
Acknowledgments
We acknowledge the University of Zimbabwe Department of Primary Health Care Sciences: Family Medicine, Global and Public Health Unit for coordinating and facilitating material support in coming up with this manuscript. The authors also acknowledge Tsitsi Patience Juru, and Dr Addmore Chadambuka, for their active participation and support in topic formulation, data collection and writing and reviewing this manuscript.
Tables and figures
Table 1: Bivariate analysis of predictors of time to viral load suppression in young people in Gwanda District, Zimbabwe, 2021
Table 2: Multivariate analysis of predictors of time to viral load suppression in young people in Gwanda District, Zimbabwe, 2021
Figure 1: Schematic presentation of data extraction of predictors of viral load suppression in young people years
Figure 2: Survival curves on time to viral suppression for young people in Gwanda, Zimbabwe, 2021
References
- WHO. WHO fact sheet on HIV/AIDS [Internet]. Geneva (Switzerland): WHO; 2024 Jul 22 [cited 2024 Nov 15].
- WHO. HIV data and statistics: Global data [Internet]. Geneva (Switzerland): WHO; [date unknown] [cited 2024 Nov 15].
- UNAIDS. Global HIV & AIDS statistics - Fact sheet [Internet]. Geneva (Switzerland): UNAIDS; 2024 [cited 2024 Nov 15]. 6 p. Download UNAIDS_FactSheet_en.pdf.
- Ministry of Health and Child Care (MoHCC) (ZW). Zimbabwe Population-based HIV Impact Assessment 2020 (ZIMPHI 2020): Final report [Internet]. Harare (ZW): (MoHCC) (ZW); 2021 Feb [cited 2024 Nov 15]. 207 p. Download 010923_ZIMPHIA2020-interactive-versionFinal.pdf.
- UNAIDS. Ending AIDS: progress towards the 90-90-90 targets [Internet]. Geneva (Switzerland): UNAIDS; 2017 [cited 2024 Nov 15]. 196 p. (2017 Global AIDS update). Report No.: UNAIDS/JC2900E. Download Global_AIDS_update_2017_en.pdf.
- UNAIDS. Young people and HIV [Internet]. Geneva (Switzerland): UNAIDS; 2021 May 7 [cited 2024 Nov 15]. 16 p. Download young-people-and-hiv_en.pdf.
- The Global Fund. Audit of Global Fund Grants in Zimbabwe [Internet]. Geneva (Switzerland): The Global Fund; 2020 Mar 26 [cited 2024 Nov 15]. 24 p. French. English. Download oig_gf-oig-20-008_report_en.pdf.
- Bvochora T, Satyanarayana S, Takarinda KC, Bara H, Chonzi P, Komtenza B, Duri C, Apollo T.Enhanced adherence counselling and viral load suppression in HIV seropositive patients with an initial high viral load in Harare, Zimbabwe: Operational issues . Mor O, editor. PLoS ONE [Internet]. 2019 Feb 5 [cited 2024 Nov 15];14(2):e0211326. https://doi.org/10.1371/journal.pone.0211326 PubMed | Google Scholar
- Hussen S, Mama M, Mekonnen B, Yihune A, Shegaze M, Boti N, Shure M. Predictors of time to viral load suppression of adult PLWHIV on ART in Arba Minch General Hospital: a follow up study . Ethiop J Health Sci [Internet]. 2019 Nov 1 [cited 2024 Nov 15];29(6): 751-8. https://doi.org/10.4314/ejhs.v29i6.12 Download ajol-file-journals_449_articles_191325_submission_proof_191325-5329-485382-1-10-2019111.pdf. Google Scholar
- Atnafu GT, Moges NA, Wubie M, Gedif G.Incidence and predictors of viral load suppression after enhanced adherence counseling among HIV-positive adults in West Gojjam Zone, Amhara Region, Ethiopia . IDR [Internet]. 2022 Jan 25 [cited 2024 Nov 15]; 15:261-74. https://doi.org/10.2147/IDR.S341392 PubMed | Google Scholar
- Epalza C, Domínguez–Rodríguez S, Cervantes E, Jiménez De Ory S, Frick MA, Fortuny C, Soler–Palacín P, Prieto–Tato L, Sainz T, Carreras–Abad C, Montero Alonso M, De Zárraga Fernández MA, Ocampo A, Rojo P, Navarro ML, the Cohort of the Spanish HIV/AIDS Pediatric (CoRISpe) and Adult (CoRIS) Networks.Factors associated with late presentation for HIV care in adolescents in Spain . HIV Medicine [Internet]. 2022 Sep 30 [cited 2024 Nov 15];23(11):1195-201. https://doi.org/10.1111/hiv.13407 Google Scholar
- Mocroft A, Lundgren JD, Sabin ML, Monforte A d´Arminio, Brockmeyer N, Casabona J, Castagna A, Costagliola D, Dabis F, De Wit S, Fätkenheuer G, Furrer H, Johnson AM, Lazanas MK, Leport C, Moreno S, Obel N, Post FA, Reekie J, Reiss P, Sabin C, Skaletz-Rorowski A, Suarez-Lozano I, Torti C, Warszawski J, Zangerle R, Fabre-Colin C, Kjaer J, Chene G, Grarup J, Kirk O, Collaboration of Observational HIV Epidemiological Research Europe (COHERE) study in EuroCoord.Risk factors and outcomes for late presentation for HIV-positive persons in europe: results from the collaboration of observational HIV epidemiological research europe study(COHERE) . Sansom SL, editor. PLoS Med [Internet]. 2013 Sep 3 [cited 2024 Nov 15];10(9):e1001510. https://doi.org/10.1371/journal.pmed.1001510 PubMed | Google Scholar
- Darcis G, Lambert I, Sauvage AS, Frippiat F, Meuris C, Uurlings F, Lecomte M, Léonard P, Giot JB, Fombellida K, Vaira D, Moutschen M.Factors associated with late presentation for HIV care in a single Belgian reference center: 2006-2017 . Sci Rep [Internet]. 2018 Jun 5 [cited 2024 Nov 15];8(1):8594. https://doi.org/10.1038/s41598-018-26852-0 PubMed | Google Scholar
- Letta S, Demissie A, Oljira L, Dessie Y.Factors associated with adherence to Antiretroviral Therapy (Art) among adult people living with HIV and attending their clinical care, Eastern Ethiopia . BMC Int Health Hum Rights [Internet]. 2015 Dec 28 [cited 2024 Nov 15];15(1):33. https://doi.org/10.1186/s12914-015-0071-x Erratum in: Erratum to: Factors associated with adherence to Antiretroviral Therapy (ART) among adult people living with HIV and attending their clinical care, Eastern Ethiopia . BMC Int Health Hum Rights [Internet]. 2016 Mar 2 [cited 2024 Nov 25];16(1):8. https://doi.org/10.1186/s12914-016-0078-y PubMed | Google Scholar
- Mosisa Y, Ewunetu A, Duftu KB, Biru B, Diriba D, Shama AT, Lemi M, Fetensa G, Feyisa BR.Predictors of HIV viral load suppression after enhanced adherence counseling, Nekemte, Ethiopia . J Epidemiol Glob Health [Internet]. 2024 May 22 [cited 2024 Nov 15];14(3):1004-11. https://doi.org/10.1007/s44197-024-00246-0 PubMed | Google Scholar
- Bisetegn G, Arefaynie M, Mohammed A, Fentaw Z, Muche A, Dewau R, Seid Y. Predictors of virological failure after adherence-enhancement counseling among first-line adults living with HIV/AIDS in Kombolcha Town, Northeast Ethiopia. HIV [Internet]. 2021 Jan [cited 2024 Nov 15]; 13:91-7. https://doi.org/10.2147/HIV.S290531 PubMed | Google Scholar
- Nyika H, Mugurungi O, Shambira G, Gombe NT, Bangure D, Mungati M, Tshimanga M. Factors associated with late presentation for HIV/AIDS care in Harare City, Zimbabwe, 2015 . BMC Public Health [Internet]. 2016 May 3 [cited 2024 Nov 15];16(1):369. https://doi.org/10.1186/s12889-016-3044-7 PubMed | Google Scholar
- Bulage L, Ssewanyana I, Nankabirwa V, Nsubuga F, Kihembo C, Pande G, Ario AR, Matovu JK, Wanyenze RK, Kiyaga C.Factors associated with virological non-suppression among HIV-positive patients on antiretroviral therapy in uganda, august 2014-july 2015 . BMC Infect Dis [Internet]. 2017 May 3 [cited 2024 Nov 15];17(1):326. https://doi.org/10.1186/s12879-017-2428-3 PubMed | Google Scholar
- Sithole Z, Mbizvo E, Chonzi P, Mungati M, Juru TP, Shambira G, Gombe NT, Tshimanga M. Virological failure among adolescents on ART, Harare City, 2017- a case-control study . BMC Infect Dis [Internet]. 2018 Sep 18 [cited 2024 Nov 15];18(1):469. https://doi.org/10.1186/s12879-018-3372-6 PubMed | Google Scholar