Assessment of factors associated with mortality among tuberculosis patients attending Muhima District Hospital, Rwanda, 2015-2018
Kamayirese Eric Noël1,&, Mukamurigo Judith2, Birungi Francine2, Sinayobye Jean d’Amour3, Ntabanganyimana Daniel4,5
1Department of Epidemiology and Biostatistics, University of Rwanda, 2School of Public Health, University of Rwanda, Kigali, Rwanda, 3African Field Epidemiology Network, Kigali, Rwanda, 4Department of Epidemiology and Biostatistics, University of Rwanda, Kigali, Rwanda, 5Ministry of Health, Kigali, Rwanda
&Corresponding author
Kamayirese Eric Noël, Department of Epidemiology and Biostatistics, University of Rwanda, Kigali, Rwanda.
Introduction:
Globally, Tuberculosis is a very serious public health problem. It is ranked as one of the ten top killer diseases worldwide. WHO estimated eight million cases were recorded in 2019, with two million related deaths every year. TB is a curable disease if the treatment is available and well followed up on with help in monitoring and evaluation of TB control program as major indicator.
Methods:
A retrospective study was conducted to assess the factors associated with TB mortality during treatment to determine the associated factors. Descriptive statistic and analytical statistics were used to compare demographic, patient behavior and clinical characteristics.
Results:
A total 445 registered TB patients with full complete information were included. Among them 74.83% were male, 4.94% died while were under treatment; 70.56%were aged 20 to 40 years old; 60.9% were married, 33.26% were single; the widowers were 23(5.17%) and the divorced 0.67%. 421(94.61%) were from urban areas. 42.92%, bivariate analysis showed that being a widower (OR 0.02; CI 0.00- 0.20) was significant, illiteracy and being educated at primary level were also significant (OR 0.86; CI 0.001- 0.019), (OR 0.05; CI 0.00-0.01) respectively; the adjusted odd ratio shows widowers (AOR: 0.01; 95% CI: 0.00 - 0.07; p = 0.001), are less likely to die while taking TB treatment compared with the married peoples and illiterate people or those having primary level education were less likely to be associated with tuberculosis mortality (AOR: 0.07; 95% CI: 0.01 – 0.45; p < 0.005), (AOR: 0.03; 95% CI: 0.00 – 0.18; p < 0.001). Therefore, illiterate people and those with primary level; both two were less likely to die compared to the reference group with TB.
Conclusion:
The tuberculosis mortality at Muhima District Hospital in the period of the study was 4.94%, lower than national rate of 6.0%, being a widower and having a low level of education and illiteracy were found as the factors associated with TB mortality. The study highlights the need for special attention to be given to the groups cited above in order to increase the adherence to the treatment and assess others factors necessary to reduce mortality due to TB not revealed by the study.
Introduction

Tuberculosis (TB) remains a serious public health problem and one of the top killer diseases worldwide, with an estimated eight million new cases with two millions of deaths every year [1-4]. A total of 10 million people were diagnosed as active TB cases in 2019, of these, an estimated 1.2 million died from TB infection with negative HIV tests, 208,000 people also died among the HIV positive cases, adults people made up 88% of recorded cases in the same year. The WHO report in South-East Asia (44%), Africa (25%), and the Western Pacific (18%) had the most people with TB. Eight countries accounted for two thirds of the global total: India (26%), Indonesia (8.5%), China (8.4%), the Philippines (6.0%), Pakistan (5.7%), Nigeria (4.4%), Bangladesh (3.6%) and South Africa (3.6%) [5].
The study, done in Southern Ethiopia on factors associated with poor tuberculosis treatment outcomes, showed that in total of 404 patients recorded in the period of study, 6.7% deaths were recorded, with higher mortality among young and old patients (aged <5 and >65 years) [
6]. The African Region continues to bear a significant proportion of the global burden of tuberculosis and accounts for 28% of the estimated 9.6 million incident tuberculosis cases that occurred worldwide in 2014 [
7].
In Africa, the TB mortality burden is increased with the human immunodeficiency virus (HIV) infection, which allows a huge number of people already have latent tuberculosis to progress to active TB infection; in some African countries where more than 60% of HIV infected persons are found, this increases exponential tuberculosis infections over recent years [
8].
The African region has also achieved a 37% decline in the TB mortality rate from 2000 to 2014 and 47% among people living with HIV. The Stop TB Strategy target of 85% treatment success rate by 2015 was achieved by 21 Member States, while the regional average stands at 79% [
9].
However, given that most deaths from tuberculosis are preventable, it is still unacceptable and many efforts to combat TB have been accelerated beyond the Millennium Development Goals (MDGs) targets, in line with recently set Sustainable Development Goal (SDGs) and the end of TB strategy targets. [
10]. By 2030, the target is to reduce the TB mortality to 95% compared with 2015 of 6 million new cases of TB notified to World Health Organization [
9].
Treatment outcome is an important indicator of any TB control program; it is also used in patient monitoring and follow-up because if the treatment fails, the patient is more likely to die or develop drug resistant tuberculosis, making it very important to assess and understand the factors associated with poor treatment outcomes of TB and take appropriate preventive measures [
11].
The early tuberculosis diagnosis accompanied with first-line treatment for six months will completely cure TB and stop the TB transmission [
12]. The reduction of health-related risk factors for TB (e.g. smoking, diabetes and HIV infection) will reduce the incidence and prevalence of TB as well as preventive treatment of people with latent TB infection, in addition to taking multi-sectoral action on broader determinants of TB infection and disease (e.g. poverty, housing quality and undernutrition) [
13].
WHO recommends that the treatment should be intensive under direct observation of the patient, and should be done in two phases; phase one of six months where the patient has to take drugs under Direct observation treatment (DOT) for the first two months [
14].
TB treatment outcome is classified into two main groups; successful TB treatment (cured) and unsuccessful TB treatment (treatment failure, treatment defaulters (anti-tuberculosis treatment discontinuation), transferred out and death [
15,
16].
TB treatment defaulters are defined as the treatment interruptions at two months following the TB treatment initiation. TB treatment failure case is one that continues to be sputum positive after five months of adequate chemotherapy. A relapse is a patient who was once declared cured but later again became sputum positive [
17]. WHO estimates of Rwanda TB burden were reduced in 2014 after the national TB prevalence survey found a lower TB prevalence than had been previously estimated [
18].
Estimated TB incidence rates in Rwanda are lower than the Global and AFRO Regional average, but remain high with 56 (48-65) incident TB cases -new and relapse-per 100,000 habitants in Rwanda in 2015 vs. 142 and 275 respectively at global and AFRO Region level.
Rwanda achieved the MDG target of halting the TB incidence in 2006. Incidence has since then been on a steady decline at an average rate of 8% per year between 2010 and 2015.
Similarly, after an initial increase between 2006 and 2010, mortality has been on a consistent decline thereafter to the current level of 6.2 per 100,000 populations [
18].
Therefore, a study on assessment of factors associated with tuberculosis mortality among tuberculosis patients attending Muhima District Hospital, Rwanda, from 2015-2018 was carried out, in order to improve the TB treatment outcomes by preventing death and drug resistance among the patients under TB treatment; the researchers, the policy makers and TB program in general will also have enough information on unfavorable TB treatment outcomes to be used used in future research, future protocol and guideline development.
Even through the Rwandan Tuberculosis (TB) program is well organized and complies with the WHO recommendation for six months of TB treatment, some patients end up with unsuccessful TB treatment outcomes. TB annual report done in Rwanda (2019); shows that unsuccessful TB treatment (death) represents 5.5% of bacteriological confirmed cases new and relapse while the clinical diagnosed cases represents 16.4% [
19].
Muhima District Hospital is one of the health facilities with unfavorable TB treatment outcomes but no study was done to assess contributing factors. In July 2015, WHO recommended use of the TB Direct Observation Treatment (TB-DOT) to increase the adherence to full course TB treatment in order to avoid unfavorable TB treatment outcome and prevent the development of drug resistance [
20].
The main objective of this study was to assess TB treatment outcomes and determine factors associated with mortality among TB patients attending Muhima DH from January 1 2015 to 31 December 2018, Kigali-Rwanda.
Methods

Study setting
The study was carried out in Muhima District Hospital, which is one of the forty-two District Hospitals in Rwanda, localized in Kigali City, Nyarugenge District in Muhima Sector, where it serves eleven health centers with a total population of 289,435. Muhima DH is a TB Center for Diagnosis and treatment (CDT) where it serves four Centers for treatment.
Study design and recruitment of study participants
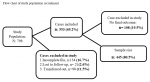
The study was a retrospective cross-sectional study including all patients who´d undergone TB treatment in Muhima DH in the period of three years (January 2015 to December 2018), aiming to determine the factors associated with tuberculosis mortality among the clients received in TB service by reviewing the characteristics of all cases of patients that died from pulmonary tuberculosis at Muhima District Hospital from January 2015 to December 2018. A total of 523 patients were used from the 798 total number of patients recorded in TB registers (See flowchart for details).
Inclusion & Exclusion criteria
This study included all patients diagnosed with pulmonary TB using standard laboratory tests and completed their six months of tuberculosis treatment at Muhima DH between January 2015 and December 2018 (
Figure 1).
Data collection
A structured excel sheet, developed using the list of interested variables by the study team, included sociodemographic characteristics such as age, sex, location, body mass index, marital status, religion, occupation, education level and some clinical variables (Serological status, treatment phase, comorbidity), the patient´s behavior (use of alcohol or smoking), localization, religion and socio-economic class so called “ubudehe category” [
21] .
In addition, the excel sheet includes clinical variables: TB regimen, serological status and treatment outcomes (date ending TB treatment, cured, died, treatment failed, lost to follow up), by trained personnel, but the positive cases were tracked using the treatment register to check treatment outcomes and other factors being used in this study.
Descriptions of variables
Variables related to TB treatment final outcomes: The outcome was a binary variable with two options; death due to Pulmonary tuberculosis and successful TB treatment (patient is alive after six months of treatment). These variables were collected from patient files.
Variables related to socio-demographic factors: age, a continuous numerical variable, was organized into 4 groups, Patients below 19 years old and the group above 60 years were classified as the groups with poor treatment outcomes while the two groups left were young people (ages 20-40) and the older group with people aged 41-60 years.
The gender of participants is a dichotomous variable where we have female and male and their marital statuses, a variable classified into four categories, (divorced, married, single and widowed). Geographical location; a participant´s location is also a dichotomous variable with both rural and urban areas. Religion was classified into four religious groups including ADEPR, which stands for all churches other than Catholic, Adventist and Islam. The education variable was grouped into four categories including the illiterate (no formal education) primary level completed, secondary level and University level.
Variables related to clinical factors: Treatment phase with phase one and phase two. Patient behavior was dichotomous where No (not smoking or not drink alcohol) and Yes (smoking or use alcohol). Comorbidity: a dichotomous variable where Yes stands for comorbidity present and No for absence of comorbidity. Serological status was a dichotomous variable with Negative and positive results. Body mass index was a variable with three categories; underweight, normal weight and overweight.
Data analysis
A descriptive analysis has been used to determine the frequencies of the different variables. The bivariate of socio-demographic factors, clinical factors and patient´s behaviors were performed to describe the study outcome. The Chi-square test (Chi´s test) showing the frequencies and crude odds ratio at 95% confidence interval were analyzed to assess the bivariate association between independent and dependent variables which was significant and determined the magnitude of association.
Then logistic regression model was used to examine the contribution to each and every independent variable to determine the death that may occur during TB treatment. Finally, the multivariate analysis model was applied on the significant variables determined in the bivariate model to control the confounding factors. Those were found at p-value of 0.05 and were shown in the results tables.
Ethical Consideration
The permission to use the data was granted from the Ethical committee at Muhima Hospital.Confidentiality was guaranteed, no personal data was released or disclosed outside of this work purpose and a unique identifier was used instead of names. However, this was considered programmatic work and no ethical clearance was therefore needed.
Results
The study sample was 445 out 798 (55.7%) of the total TB patients from the hospital´s TB documents where 24 (5.3%) died; while they were under TB treatment and 421 (94.6%) had successful TB treatment outcomes. This a small number compared to a retrospective study of the profile and treatment outcomes of all tuberculosis patients in a five- year period study conducted at Gondar University Teaching Hospital in Northwest Ethiopia which shows that this was an unsatisfactory result; the treatment success rate of all tuberculosis cases was 29.5% which might be collated with death rate of 10.1% [22].
Males represented a big number of the patients with 313 (74.8%) patients. Females represented 112 (25.1%), of the participants. The age the group of 20 to 40 years old were represented by 314 (70.3%) of the total number of patients; the 35 to 43 year old group were represented by 140 patients (31.4%); the patients who were younger than or equal to 25 years old were 87 (19.5%) and those above 44 years were 79 (17.7%); the marital status of patients showed that 282 (63.3%) were married, 148(33.2%) were single; 15 (3.3%) were widowed or divorced; geographical location showed that 403 (90.5%) were from urban area and 42 (9.4%) from rural areas. 214 (48.1%) patients represented the Catholic church, ADEPR had 201 (45.1%) patients and 30 (6.7%) were Islam.
The patients with secondary school level education were 296 (66.52%), those with primary level education were 93 (20.9%), those who did not attend school at all were 47(10.56%) and those with university level education were 9(2.02%); the private sector (traders, bank agents, etc.) were represented by 195 (43.82%) patients; unemployed patients were 124 (27.87%) the public sector (public employees) were represented by 74 (16.62%) and transportation staffs were 52 (11.68%).
The patients with diabetes were 26 (5.84%), HIV positive patients were 168 (37.75), hepatitis patients were 12 (2,69%) and 239 (53.70%) had no other comorbidity. The serological status in the patients was as follows: 277(62.25%) were HIV negative and 168(37.75%) were HIV positive. Patient´s behaviors: 431(97.53) did not smoke, 11(2.47%) were smokers, 363(81.57%) did not use alcohol and 82 (18.43%) did (
Table 1).
The findings from bivariate analysis (
Table 2) shows that three variables out of eleven were significant to die while a patient is under TB treatment including marital status (p value 0.001), education level (p value 0.001) and having comorbidity (p value 0.002). All other variables were not significant (
Table 2).
The adjusted risk factors of TB treatment outcomes are presented in
Table 3. The logistic regression model showed that being widower was less likely associated with TB treatment outcome (death due to TB) (AOR: 0.05; 95% CI: 0.00 - 0.10; p = 0.001); widowers are less likely to die while taking TB treatment compared to the married people. Those who had the secondary school level education were more likely to die while taking anti-TB 19.7 times more than those who did primary school level only (AOR: 18.7; 95% CI; (5.00-70.01) and those who have a comorbidity such as Hepatitis were less likely to die compared to the reference group with TB (p < 0.005, AOR: 0.01; 95% CI: 0.00 - 0.11) (
Table 3).
Discussion
This retrospective document review on TB treatment outcomes, a primary data analysis done at Muhima District Hospital from January 2015 to December 2018, shows that the majority of patients were male (70.33%), (63.37%) were married and (66.51%) reached secondary school education level. Those findings are similar to other studies done in Harar Town, Eastern Ethiopia where males represents 59.8% and 3.9% died while taking anti-tuberculosis treatment [23].
In this study the unfavorable TB treatment outcome was 5.4% (24/445), which was low compared to the national outcome of of 6.9% [
1]. The successful treatment outcome was 94.6% (421/445), this very low compared with the unfavorable at Jinka General Hospital, southern Ethiopia by Beniam Wondale where among 60.9% of complete treatment, 10.2% [
24]; almost third of patients were male 74.84% while 25.17% were male. This in concordance with the tuberculosis epidemiology as males are more exposed to infection in community than females, the occupational and psycho-social effect with may prevent the female not contracting the tuberculosis [
25].
The bivariate analysis shows that widowers were at risk to die while taking TB treatment than married people (OR 0.05; CI 0.00- 0.10); being illiterate (OR 0.86; CI 0.001- 0.019) and being educated at primary level (OR 0.05; CI 0.00- 0.01); this is almost too similar of the cohort study done in Brazil from May 2001 to July 2003 where the main factors associated with tuberculosis mortality were age group, HIV coinfection, illiteracy and prior TB treatment [
26].
The adjusted risk factors of TB treatment outcome the logistic regression model being widower was significant associated with TB treatment outcome (AOR: 0.01; 95% CI: 0.00 - 0.07; p = 0.001), the status of being widowers increases the risk of die with TB treatment under treatment compared to married peoples as reference. Being illiterate or having primary level were also statistically significant associated with tuberculosis mortality (AOR: 0.07; 95% CI: 0.01 - 0.45; p < 0.005), (AOR: 0.03; 95% CI: 0.00 - 0.18; p < 0.001) respectively so illiterate people and those with primary level were less likely to die with TB compared to those with secondary level.
This is similar to a case control study done in public health institution in Eastern of Ethiopia where the evaluation of factors associated with tuberculosis mortality: age, gender, presence of contact person, treatment category and HIV sero-status were found to be associated with one high risk of that poor outcome as lack of contact person to be contact while the patient is under treatment with (AOR 1.37; 95% CI 1.14-2.91, P=0.024) [
27].
Conclusion
The data of this study revealed that the tuberculosis mortality at Muhima District Hospital was 5.4% it was lower than national rate of 6.9% in 2019. The study suggests that the factors associated with TB mortality were marital status (widowers) and level of education (illiterate and primary level). Our study emphasizes on a special attention to the groups cited above in order to increase the adherence of treatment and assessing the others factors not revealed by the present study to reduce the mortality due to TB.
Recommendations
The retrospective document review was our design to collect all data on different variables susceptible of being the associated factors of TB treatment outcome at Muhima District Hospital but the registers were not complete and the important needed variables were missing such treatment outcome, serological status, occupation, height and weight.
The study recommends to Muhima tuberculosis clinical to record all information on TB treatment patients file and to review the filing model and the researcher also recommend to conduct other studies in different regions across country.
What is known about this topic
- TB is a deathly disease worldwide especially in under developed countries
- HIV co-infection contributes significantly to TB mortality
What this study adds
- Lonely people and those with higher education levels were associated with TB mortality. Health care providers should therefore pay attention to these groups during the treatment period
Competing interests
The authors declare no competing interests.
Authors' contributions
Protocol development: K.E.N, M.J. Methodology: K.E.N, M.J, S.J.A. Data analysis: K.E.N, S.J.A, N.D. Validation: M.J, S.J.A, N.D. Manuscript writing: review & editing: K.E.N, B.F, S.J.A, M.J. Supervisor: B.F. All authors read and approved final version of the manuscript.
Acknowledgments
We are thankful to Muhima hospital upper management and to Muhima hospital TB focal person who supported to get data from the health facilities records. We are also grateful to the University of Rwanda and African Field Epidemiology unevaluable support to carry out the present study and to the Muhima Hospital laboratory staffs and staffs working in Tuberculosis service for heling us in data collection.
Tables and figures
Table 1: Frequency of socio-demographic characteristics recorded in TB cases registers (n=445) at Muhima District Hospital, Kigali-Rwanda,2015-2018
Table 2: Association between TB treatment outcome and socio-demographic characteristics of the study participants (Bivariate analysis) Kigali-Rwanda, 2015-2018
Table 3: Multivariate logistic regression analysis of significant risk factors of TB treatment outcome according to clinical characteristic of TB patients at Muhima District Hospital, Kigali-Rwanda 2015-2018
Figure 1: Overview of Case inclusion in study
References
- Ministry of Health (RW). National Tuberculosis and Other Respiratory Communicable Diseases Program: Annual Report 2019-2020 [Internet]. Kigali (Rwanda): Rwanda Biomedical Centre; 2019 May 14 [cited 2023 Sep 24]. 83 p.
- World Health Organization. Global Tuberculosis report 2019 [Internet]. Geneva (Switzerland): WHO; 2019 [cited 2023 Sep 24]. 297 p.
- Blomberg B, Spinaci S, Fourie B, Laing R.The rationale for recommending fixed-dose combination tablets for treatment of tuberculosis . Bull World Health Organ[Internet]. 2001 [cited 2023 Sep 24];79(1):61-8. Download PMC2566330.pdf. Google Scholar
- World Health Organization. Global tuberculosis report 2020 [Internet]. Geneva (Switzerland): WHO; 2020 Oct 15 [cited 2023 Sep 19]. 232 p.
- Chakaya J, Khan M, Ntoumi F, Aklillu E, Fatima R, Mwaba P, Kapata N, Mfinanga S, Hasnain SE, Katoto PDMC, Bulabula ANH, Sam-Agudu NA, Nachega JB, Tiberi S, McHugh TD, Abubakar I, Zumla A.Global Tuberculosis Report 2020 - Reflections on the Global TB burden, treatment and prevention efforts . International Journal of Infectious Diseases [Internet]. 2021 Mar 11 [cited 2023 Sep 19];113(Suppl 1):S7-S12 https://doi.org/10.1016/j.ijid.2021.02.107 PubMed | Google Scholar
- Muñoz-Sellart M, Cuevas LE, Tumato M, Merid Y, Yassin MA.Factors associated with poor tuberculosis treatment outcome in the Southern Region of Ethiopia. Int J Tuberc Lung Dis [Internet]. 2010 Aug 1 [cited 2023 Sep 19];14(8):973-9. Google Scholar
- WHO. Global Tuberculosis Report 2014 [Internet]. Geneva (Switzerland): WHO; 2014 Oct 23 [cited 2023 Sep 19]. 171 p.
- Khunthason S, Kaewkungwal J, Pan-Ngum W, Okascharoen C, Apidechkul T, Lawpoolsri S.The Factors associated with the unsuccessful tuberculosis treatment of hill tribe patients in Thailand. J Infect Dev Ctries [Internet]. 2020 Jan 31 [cited 2023 Sep 19];14(01):42-7. https://doi.org/10.3855/jidc.12029 Google Scholar
- World Health Organization Regional Office for Africa. End TB by 2030: Framework for implementing the “End TB Strategy” in the African region 2016 - 2020 [Internet]. Brazaville (Republic of Congo): World Health Organization Regional Office for Africa; 2017 [cited 2023 Sep 19]. 28 p. Download TBstrat-eng.pdf Google Scholar
- World Health Organization. The End TB Strategy [Internet]. Geneva (Switzerland): WHO; 2015 Aug 16 [cited 2023 Sep 19]. 20 p. Download WHO-HTM-TB-2015.19-eng.pdf WHO Reference Number: WHO/HTM/TB/2015.19 Google Scholar
- Kyu HH, Maddison ER, Henry NJ, Mumford JE, Barber R, Shields C, Brown JC, Nguyen G, Carter A, Wolock TM, Wang H, Liu PY, Reitsma M, Ross JM, Abajobir AA, Abate KH, Abbas K, Abera M, Abera SF, Abera Hareri H, Ahmed M, Alene KA, Alvis-Guzman N, Amo-Adjei J, Andrews J, Ansari H, Antonio CA, Anwari P, Asayesh H, Atey TM, Atre S, Barac A, Beardsley J, Bedi N, Bensenor I, Beyene AS, Butt ZA, Cardona PJ, Christopher D, Dandona L, Dandona R, Deribe K, Deribew A, Ehrenkranz R, El Sayed Zaki M, Endries A, Feyissa TR, Fischer F, Gai R, Garcia-Basteiro AL, Gebrehiwot TT, Gesesew H, Getahun B, Gona P, Goodridge A, Gugnani H, Haghparast-Bidgoli H, Hailu GB, Hassen HY, Hilawe E, Horita N, Jacobsen KH, Jonas JB, Kasaeian A, Kedir MS, Kemmer L, Khader Y, Khan E, Khang YH, Khoja AT, Kim YJ, Koul P, Koyanagi A, Krohn KJ, Kumar GA, Kutz M, Lodha R, Magdy And El Razek H, Majdzadeh R, Manyazewal T, Memish Z, Mendoza W, Mezgebe HB, Mohammed S, Ogbo FA, Oh IH, Oren E, Osgood-Zimmerman A, Pereira D, Plass D, Pourmalek F, Qorbani M, Rafay A, Rahman M, Rai RK, Rao PC, Ray SE, Reiner R, Reinig N, Safiri S, Salomon JA, Sandar L, Sartorius B, Shamsizadeh M, Shey M, Shifti DM, Shore H, Singh J, Sreeramareddy CT, Swaminathan S, Swartz SJ, Tadese F, Tedla BA, Tegegne BS, Tessema B, Topor-Madry R, Ukwaja KN, Uthman OA, Vlassov V, Vollset SE, Wakayo T, Weldegebreal S, Westerman R, Workicho A, Yonemoto N, Yoon SJ, Yotebieng M, Naghavi M, Hay SI, Vos T, Murray CJ. The global burden of tuberculosis: results from the Global Burden of Disease Study 2015. The Lancet Infectious Diseases [Internet]. 2017 Dec 6 [cited 2023 Sep 19];18(3):261-84. https://doi.org/10.1016/s1473-3099(17)30703-x Google Scholar
- Rockwood N, Du Bruyn E, Morris T, Wilkinson RJ.Assessment of treatment response in tuberculosis. Expert Review of Respiratory Medicine [Internet]. 2016 Mar 31 [cited 2023 Sep 19];10(6):643-54. https://doi.org/10.1586/17476348.2016.1166960 PubMed | Google Scholar
- Lakoh S, Jiba DF, Adekanmbi O, Poveda E, Sahr F, Deen GF, Foray LM, Gashau W, Hoffmann CJ, Salata RA, Yendewa GA.Diagnosis and treatment outcomes of adult tuberculosis in an urban setting with high HIV prevalence in Sierra Leone: A retrospective study. International Journal of Infectious Diseases [Internet]. 2020 Apr 24 [cited 2023 Sep 19];96:112-18. https://doi.org/10.1016/j.ijid.2020.04.038 Google Scholar
- World Health Organization. What is DOTS? A Guide to Understanding the WHO-recommended TB Control Strategy Known as DOTS [Internet]. Geneva (Switzerland): WHO; 1999 [cited 2023 Sep 19]:33 p. Document Number:WHO/CDS/CPC/TB/99.270 Google Scholar
- Anuwatnonthakate A, Limsomboon P, Nateniyom S, Wattanaamornkiat W, Komsakorn S, Moolphate S, Chiengsorn N, Kaewsa-ard S, Sombat P, Siangphoe U, Mock PA, Varma JK.Directly observed therapy and improved tuberculosis treatment outcomes in thailand. Maartens G, editor. PLoS ONE [Internet]. 2008 Aug 28 [cited 2023 Sep 19];3(8):e3089. https://doi.org/10.1371/journal.pone.0003089 PubMed | Google Scholar
- Johnson W, Onuma O, Owolabi M, Sachdev S.Stroke: a global response is needed . Bull World Health Organ [Internet]. 2016 Sep 1 [cited 2023 Sep 19];94(9):634-634A. https://doi.org/10.2471/blt.181636 PubMed | Google Scholar
- Dooley KE, Lahlou O, Ghali I, Knudsen J, Elmessaoudi MD, Cherkaoui I, El Aouad R.Risk factors for tuberculosis treatment failure, default, or relapse and outcomes of retreatment in Morocco . BMC Public Health [Internet]. 2011 Feb 28 [cited 2023 Sep 19];11(1):140. https://doi.org/10.1186/1471-2458-11-140 PubMed | Google Scholar
- Migambi P, Gasana M, Uwizeye CB, Kamanzi E, Ndahindwa V, Kalisvaart N, Klinkenberg E.Prevalence of tuberculosis in Rwanda: Results of the first nationwide survey in 2012 yielded important lessons for TB control . PLOS ONE [Internet]. 2020 Apr 23 [cited 2023 Sep 19];15(4):e0231372. http://dx.doi.org/10.1371/journal.pone.0231372 PubMed | Google Scholar
- Ministry of Health (RW). National Tuberculosis and other respiratory communicable Diseases Program Annual Report 2018-2019 [Internet]. Kigali (Rwanda): Rwanda Biomedical Centre; 2019 [cited 2023 Sep 19]. 50 p.
- McLaren ZM, Milliken AA, Meyer AJ, Sharp AR.Does directly observed therapy improve tuberculosis treatment? More evidence is needed to guide tuberculosis policy. BMC Infectious Diseases [Internet]. 2016 Oct 4 [cited 2023 Sep 19];16(1):537. http://dx.doi.org/10.1186/s12879-016-1862-y PubMed | Google Scholar
- Nizeyimana P, Lee KW, Sim S.A study on the classfication of households in Rwanda based on factor scores. Journal of the Korean Data & Information Science Society [Internet]. 2018 Mar 31 [cited 2023 Sep 19];29(2):547-55. http://dx.doi.org/10.7465/jkdi.2018.29.2.547 Download JKDISS029-02-19.pdf. Google Scholar
- Tessema B, Muche A, Bekele A, Reissig D, Emmrich F, Sack U. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia. A five - year retrospective study. BMC Public Health [Internet]. 2009 Oct 4 [cited 2023 Sep 19];9(1):371-8. https://doi.org/10.1186/1471-2458-9-371 PubMed | Google Scholar
- Tola A, Minshore KM, Ayele Y, Mekuria AN.Tuberculosis treatment outcomes and associated factors among tb patients attending public hospitals in harar town, eastern ethiopia: a five-year retrospective study . Tuberculosis Research and Treatment [Internet]. 2019 Apr 1 [cited 2023 Sep 19];2019: 1503219. https://doi.org/10.1155/2019/1503219 PubMed | Google Scholar
- Wondale B, Medihn G, Teklu T, Mersha W, Tamirat M, Ameni G.A retrospective study on tuberculosis treatment outcomes at Jinka General Hospital, southern Ethiopia. BMC Res Notes [Internet]. 2017 Dec 4 [cited 2023 Sep 19];10(1):680. https://doi.org/10.1186/s13104-017-3020-z PubMed | Google Scholar
- El-Shabrawy M, El-Shafei DA.Evaluation of treatment failure outcome and its predictors among pulmonary tuberculosis patients in Sharkia Governorate, 2013-2014 . Egyptian Journal of Chest Diseases and Tuberculosis [Internet]. 2016 Sep 28 [cited 2023 Sep 19];66(1):145-52. https://doi.org/10.1016/j.ejcdt.2015.11.002 Google Scholar
- Albuquerque MDFPMD, Ximenes RADA, Lucena-Silva N, Souza WVD, Dantas AT, Dantas OMS, Rodrigues LC.Factors associated with treatment failure, dropout, and death in a cohort of tuberculosis patients in Recife, Pernambuco State, Brazil . Cad Saúde Pública [Internet]. 2007 May 31 [cited 2023 Sep 19];23(7):1573-82. https://doi.org/10.1590/s0102-311x2007000700008 Google Scholar
- Amante TD, Abdosh T.Risk factors for unsuccessful tuberculosis treatment outcome (Failure, default and death) in public health institutions, Easter Ethiopia . Pan Afr Med J [Internet]. 2015 Mar 16 [cited 2023 Sep 19];20:247 https://doi.org/10.11604/pamj.2015.20.247.3345 PubMed | Google Scholar