Factors associated with contracting SARS-COV2 in Bikita District, Zimbabwe, 2021
Hellen Kabaya1,2, Emmanuel Govha1, Bernard Madzima2, Tsitsi Juru1,&, Notion Gombe1,3, Maurice Owiny4, Mufuta Tshimanga1
1University of Zimbabwe, Department of Primary Health Care Sciences Global and Public Health Unit, Harare, Zimbabwe, 2National AIDS Council of Zimbabwe, Harare, Zimbabwe, 3African Field Epidemiology Network, Harare, Zimbabwe, 4African Field Epidemiology Network, Nairobi, Kenya
&Corresponding author
Tsitsi Juru, University of Zimbabwe, Department of Primary Health Care Sciences Global and Public Health Unit, Harare, Zimbabwe. tsitsijuru@gmail.com
Introduction:
COVID-19 (Coronavirus disease, 2019) is an infectious respiratory illness caused by severe acute respiratory syndrome‐Corona Virus2 (SARS-CoV2). As of January 8, 2021, Zimbabwe had 19660 cases. Bikita district recorded its first community acquired SARS-COV2 case on December 18, 2020, a daughter to an imported case from South Africa. By January 30, 2021, cases had risen to 221. We conducted a case-control study to determine factors associated with contracting SARS-COV2 in Bikita.
Methods:
We recruited 90 case-control pairs. Most cases were males, 52 (58%). The median age of cases was 36 (Q1=12; Q3=74) and of the controls was 38 (Q1=12; Q3=75). The independent factors associated with contracting SARS-COV2 in Bikita were attending a gathering (aOR:2.03,95%CI:1.07‐5.34), sharing sleeping spaces (aOR:1.68;95%CI:1.05‐4.87) and social distancing (aOR:0.09,95%CI:0.03‐0.48).
Results:
We recruited 90 case-control pairs. Most cases were males, 52 (58%). The median age of cases was 36 (Q1=12; Q3=74) and of the controls was 38 (Q1=12; Q3=75). The independent factors associated with contracting SARS-COV2 in Bikita were attending a gathering (aOR:2.03,95%CI:1.07‐5.34), sharing sleeping spaces (aOR:1.68;95%CI:1.05‐4.87) and social distancing (aOR:0.09,95%CI:0.03‐0.48).
Conclusion:
Independent risk factors for contracting SARS-COV2 in Bikita were attending a gathering and sharing sleeping spaces. Social distancing was protective. We recommended supervised funerals by environmental health technicians, procurement of bicycles to conduct contact tracing and health education on SARS-COV2 was given to the community.
Introduction

Coronavirus disease (COVID-19) is a new form of respiratory disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-COV2). This novel, highly infectious disease originated in Wuhan City, Hubei province, China in December 2019. In the past century, the global pandemic of COVID-19 has become the largest public health crisis. It has resulted in intimidating health, social and economic challenges [1]. Just over a year since the first known cases, COVID?19 has been linked to over 2.75 million deaths and vigorous epidemic waves have continued to spread across the globe. Despite relentless efforts for global containment, isolation and quarantine, the incidence of COVID-19 continues to rise. As of November, 30, 2021 over 260 million confirmed cases had been recorded worldwide with Africa contributing 7.6 million cases while Zimbabwe had 134652 cases [2].
Countries in the African continent have had challenges in controlling COVID-19 infections and reducing mortality rates. The continent has had weak public health delivery systems, handling large populations of vulnerable people including those immunocompromised due to coinfection with HIV/AIDS and non-communicable diseases [
3]. Zimbabwe developed a national preparedness and response plan for COVID-19 aligned to World Health Organization (WHO)´s global 2019 Novel Coronavirus Strategic Preparedness and Response Plan on January 24, 2020. This was in line with the provisions in the International Health Regulations (IHR) of 2005 [
4]. The overall goal of Zimbabwe´s national preparedness and response plan was to minimize morbidity and mortality resulting from COVID-19 and associated adverse socio-economic impact in Zimbabwe while strengthening national core capacities [
5].
The first case of community-acquired COVID-19 in Bikita district, Zimbabwe was recorded on December 18, 2020. The incidence of COVID-19 in the district rose to 221 cases by January 30, 2021. Line listing and contact tracing were conducted. The number of COVID-19 cases increased significantly causing a threat to the rural district that has a relatively large elderly population at higher risk of the severe form of the disease. The district also has limited health care facilities with only two hospitals and a shortage of health care workers in most facilities [
6]. We conducted a case-control study to determine factors associated with contracting SARS-COV2 in Bikita District.
Methods

Study design
We conducted a 1:1 unmatched case-control study. We defined a case as a person who tested SARS-COV2 positive with antigen-RDT (Rapid diagnostic test) Bikita district from December 18, 2020 to January 30, 2021.
Study setting
We conducted the study in Bikita district which is a rural district located in Masvingo Province, Zimbabwe. The population at risk of contracting SARS-COV2 was 183 184, 12.9% being above 60 years old [
7]. The district has a population density of 34.65 per square kilometer. The district had two hospitals namely Silveira and Mashoko Mission hospitals and 14 clinics. Samples for testing SARS-COV2 infection were being sent to the hospital laboratories in the district. There was a provincial quarantine facility at Nyika growth point and each health facility had a designated isolation facility for COVID-19 patients.
Study population
Our study population was residents of Bikita District who got tested for SARS-COV2 from December 18, 2020 to January 30, 2021. We defined a case as a person with a laboratory confirmed positive test for SARS-COV2 in Bikita District from 18th of December 2020 to January 30, 2021, and a control as a person with a laboratory confirmed SARS-COV2 negative test in Bikita District in the same period. Any person meeting above criteria of being a case or control willing to participate was included into the study. Those who are not available on the day of the interview and those who refused to participate in the study were excluded from the study. Key informants were the District Medical Officer, Priest-in-charge and three traditional chiefs.
Sample size calculation and sampling of study participants
We calculated sample size using Fleiss formula embedded in EPI info 7 based on a similar study done by, Farooq Phiriyasart et al, “Outbreak Investigation of COVID-19 among Islamic Missionaries in Southern Thailand, April 2020” [
8]. We assumed 50% exposure in cases, OR for attending a gathering, of 2.37, 95% confidence level, power of 80%, and 10% refusal rate, a minimum sample size of 90 cases and 90 controls was calculated.
Our sampling frame for cases was the line list of all SARS-CoV2 positive persons. Using RAND and RANK function in Microsoft Excel computer software, we randomly selected 90 cases. We created a list of people who tested negative for SARS-COV2 and that was used as the sampling frame for controls. Using the same RAND and RANK function in excel, we randomly selected our controls. All the COVID-19 case investigation forms for the selected cases were considered for review. Traditional chiefs were randomly selected using the same RAND and RANK function.
Data collection
We used a pre-tested interviewer-administered questionnaire to collect data from the study participants on socio-demographic characteristics, risk factors for contracting SARS-COV2, knowledge, attitudes and practices of COVID-19. A key informant guide was used to collect data on the general effect of COVID-19 in the district. Interviews were conducted face-to face by the public health officer using Shona language and responses recorded in English.
Data analysis
We analysed quantitative data using Epi-Info statistical software version 7 to generate frequencies and means of variables. We calculated odds ratios and their respective 95% confidence intervals. Stratified analysis was conducted to control for possible confounding and assess for possible effect modification. We used backward logistic regression to determine independent risk factors for contracting SARS-COV2. Backward logistic starts with all possible explanatory variables with p-values <0.01 and then eliminates the least statistically significant variables, one-by-one. The discarding stops when each variable remaining in the equation is statistically significant with a p-value <0.05. We carried out significant testing for statistical 5% significance of the difference in measured variables between cases and controls.
Availability of data and materials
The data sets generated and analysed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
We obtained permission to carry out the study from the Health Studies Office (HSO), Provincial Medical Director of Masvingo and the District Medical Officer of Bikita District. We obtained ethical clearance to conduct the study from HSO. We obtained informed written consent from all study participants. Confidentiality of the participants was maintained throughout the study by not using personal identifying information and data collected were used only for the study.
Results
Descriptive epidemiology
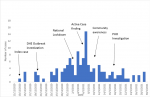
The COVID-19 outbreak in Bikita district started on December 18, 2020 when the district hospital received two symptomatic patients who tested positive for SARS-COV2. These were imported cases from South Africa. By January 30, 2021, the district had recorded 221 cases
Figure 1. Imported cases were 5/221 (2%) and the rest were local transmissions. The majority of cases, 93/221 (42%) were in the age group of 20-40 years. Only 11/221 (5%) were above 60 years and 40/221 (18%) were in the age group of <20 years. More males 121/221 (55%) were affected compared to females, 150/221 (68%) of the cases were employed, 88/150 (59%) being health care workers, 15/150 (10%) informal business traders, and only 5/150 (3%) were teachers. High school students were 18/221 (8%) of the cases. Most of the cases, 132/221 (62%) had attained secondary or tertiary level of education.
The majority of cases,179/221 (81%) were clustered around Silveira Mission Hospital, Bikita Rural Hospital and Nyika clinic. In Silveira, cases were mostly distributed in boarding facilities like the nursing homes, school hostels and at the hospital staff quarters. Sharing a sleeping place was reported by 150/221 (68%) of the cases. Cases who reported consistent hand washing were 120/221 (54%) although 157/221 (71%) had a regular water supply. Bikita´s growth point, Nyika which is the central business area with the largest beer halls in the district had 52/221 (24%) cases. Most of the cases, 179/221 (81%) admitted to having had attended gatherings and 163/221 (74%) reported a consistent use of face mask in public places. Having a visitor from South Africa or outside the district was reported by 31/221 (14%) and 121/221 (55%) of the cases had contact with a case. We therefore hypothesized that attending a gathering was a likely risk factor for contracting SARS-COV2.
The most common symptom was a runny nose, 172/221 (78%) and 51/221 (23%) cases were asymptomatic. Cases that were admitted into isolation facilities with moderate disease were 32/221 (14.4%) and 6/221 (3%) developed severe disease. Most of the cases, 182/221 (83%) self-isolated at home. Cases were managed according to the WHO guidelines. Cases that practiced steam therapy were 181/221 (82%). The commonly used herbs were zumbani tea, 168/221 (76%), lemon 61/221 (27.8%) and Mufandichimuka 37/221 (16.7%). The median days of disappearance of symptoms was 3 days (Q1=1day Q3=14 days). The recovery rate in Bikita district as of January 30, 2021 was 68% and the case fatality rate was 2.7%.
Socio-demographic characteristics of study participants
Of the 90 cases enrolled into the study, 52 (58%) were males. Males were equal to females in the control group. The median age of cases was 36 (Q1=12; Q3=74) and of the controls was 38 (Q1=12; Q3=75). Both cases and controls had 54 (60%) having attained secondary level of education. Cases who had a family size >3 were 57 (63.3%) compared to controls with 54 (60%). Cases and controls were comparable for age, gender, level of education, employment status and family size
Table 1.
Factors associated with contracting SARS-COV2 in Bikita district, 2021
The significant risk factors associated with contracting SARS-COV2 in Bikita District were attending a gathering (OR= 3.53, 95%CI: 1.87- 6.66, p=<0.01), sharing a sleeping space (OR= 2.48, 95%CI: 1.36- 4.52, p=<0.01), having a visitor from South Africa or other place outside of Bikita (OR= 3.13, 95%CI: 1.08- 9.10, p=0.03) and being employed as a healthcare worker (OR= 1.53, 95%CI: 1.08- 4.42, p=0.02). Social distancing (OR= 0.24, 95%CI: 0.10- 0.53, p=<0.01) and use of herbs (OR= 0.55, 95%CI: 0.17- 0.94, p=0.02) were significant protective factors
Table 2.
On stratified analysis, the association between attending a gathering and contracting SARS-COV2 was modified by gender. Males who attended gatherings were 3.65 times more likely to contract SARS-COV2 than those who did not attend gatherings whereas females were 2.69 times more likely to contract SARS-COV2.
On multivariate analysis, the independent risk factors for contracting SARS-COV2 in Bikita district were attending a gathering (aOR: 2.05, 95% CI: 1.07-5.34) and sharing a sleeping space (aOR: 1.68, 95% CI: 1.05-4.87). Social distancing (aOR: 0.24, 95% CI: 0.03-0.48) was an independently protective factor
Table 2.
Discussion
We found that independent risk factors for contracting SARS-COV2 in Bikita District were attending a gathering and sharing a sleeping space. The independently protective factor was social distancing. This knowledge would help us identify risk and protective factors for contracting SARS-COV2 in districts similar to Bikita that we can address to prevent further spread of this highly infectious and deadly virus.
We found that people who attended a gathering were thrice more likely to contract SARS-COV2 compared to those who did not attend gatherings. It was difficult for people who attended gatherings to maintain social distancing for example at a funeral or boarding school. This was consistent with a study done in Africa in 2020, which noted that Africa has a well-merited reputation of many daily activities on social interactions including church, market shopping, community meetings or funerals and any strategies would need to recognise these socio-cultural challenges [
9]. On further analysis, we found out that more males were attending gatherings compared to females. Males were sixty percent more likely to contract SARS-COV2 compared to females. In Bikita district, women are expected to stay at home looking after children compared to men who were more likely to attend social gatherings like cattle dip events, beer hall or ndari where there will be no social distancing or wearing of a face mask. It could also be explained by women´s cultural duties which allowed them to practice hand washing more often compared to men [
10].
We also found that people who were sharing a sleeping space were twice more likely to develop SARS-COV2 than those who did not. The risk of transmission was high as there were a cohort of student nurses who were sharing a sleeping space (4 per room) and overlapping duties for the healthcare workers. According to WHO, the airborne transmission was noted to occur in poorly ventilated indoor spaces, particularly if individuals are in the same room for an extended period [
10] which is consistent with a finding of increased risk of contracting SARS-COV2 of people sharing a sleeping space in this study. Contini et al, 2020, similar to our findings noted an increase in the probability of SARS-COV2 infection in specific indoor environments, like hospitals [
11].
In addition, we found that observing social distance was significantly protective, those who observed social distancing were eighty percent less likely to contract SARS-COV2 than those who had not which was consistent with findings by Zhang et al (2020) who found out that practising social distance reduce spread of SARS-COV2 by over ninety-five percent [
12]. In this study, consultation rooms were noted to be small both at the clinics and hospital, compromising social distancing in healthcare facilities. The district also received persistent rains which promoted crowding under shelters and thereby minimising the possibility of practicing social distancing. The productive age group was the most affected as they were at more risk of being in social gatherings at work, community meetings or social events. This is in support of prioritising those above 18 years for the COVID-19 vaccination programme as they are at more risk of contracting the virus [
13].
Study limitations
The major limitation in this study was selection bias. Some parts of Bikita district could not be reached because of poor road networks. We solely relied on the participant´s responses to historical events and there were no records with our study variables thereby creating information bias. To minimize this bias, we gave a brief history of the study to our participants and assured them that their responses will not be linked to them.
Conclusion
Males and healthcare workers were most affected by SARS-COV2 in Bikita District. Independent risk factors for contracting SARS-COV2 in Bikita District were attending a gathering and sharing sleeping spaces. The independent protective factor for SARS-COV2 was maintaining social distancing. There would be a low vaccine uptake if it is to be rolled out. The district responded swiftly but was however not well prepared for the outbreak. We recommended supervised community meetings and that funerals/burials be conducted and supervised by environmental health officers, screening of patients at health facility entrances and immediate testing of probable cases before consultation, health education on the COVID-19 vaccine and further studies to determine the efficacy of non-pharmacological medicine for COVID-19.
What is known about this topic
- The outbreak of the novel COVID-19 was a threat to the health of people globally
- Human to human transmission of the severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) occurs most often when people are in the incubation stage of the disease or are carriers and have no symptoms
What this study adds
- In this study, an outbreak investigation was carried out to determine factors associated with contracting SARS-COV-2 in a rural setting and willingness to accept COVID-19 vaccines. The results showed that healthcare workers were most affected by SARS-COV2, attending a gathering was associated with contracting COVID-19 and there would be a low vaccine uptake if the COVID-19 vaccine was to be introduced.
- This study added value in coming up with tailored interventions to decrease the transmission of SARS-COV-2 in rural settings such as conducting supervised community meetings and funerals/burials by environmental health officers, screening of patients at health facility entrances, and immediate testing of probable cases before consultation and providing health education on the COVID-19 vaccine
Competing interests
We declare that we have no competing interests as the authors.
Funding
Funding for this study was given by National AIDS Council.
Authors' contributions
HK: conception, design, acquisition, analysis and interpretation of data and drafting the manuscript. BM: conception, design, acquisition, analysis and interpretation of data and drafting the manuscript. EG: conception, design, acquisition, analysis, interpretation and reviewing of several manuscript drafts for important intellectual content. EG: conception, design, acquisition, analysis and interpretation of data and reviewing manuscript draft for important intellectual content. MOO: interpretation of data and reviewing manuscript draft for important intellectual content. NTG: conception, design, acquisition, analysis and interpretation of data and reviewing manuscript draft for important intellectual content. MT: conception, design, acquisition, analysis and interpretation of data and reviewing manuscript draft for important intellectual content. The authors read and approved the final manuscript.
Acknowledgments
Our sincere gratitude goes to the staff and management of Bikita District. Special thanks go to the staff in the University of Zimbabwe, Department of primary health services and the health studies office for all the assistance rendered. Many thanks to National AIDS Council for funding this study and Bikita district residents who participated in the study. Lastly, we would like to thank fellow MPH (Masters in public health) residents and our families for the support during the project.
Tables and figures
Table 1: Demographic characteristics of cases and controls in a study done in Bikita district in 2021
Table 2: Factors associated with contracting SARS-COV2 in Bikita district in 2021
Figure 1: Distribution of covid-19 cases in Bikita district, Masvingo Province, Zimbabwe by time, 18 December2020 to 30 January 2021
References
- Centers for Disease Control and Prevention (CDC).Global COVID-19 [Internet]. Atlanta, Georgia, USA: CDC; 2020 [updated 2023 Jan 24; cited 2023 Jul 31].
- World Health Organization.WHO Coronavirus Disease (COVID-19) Dashboard [Internet]. Geneva, Switzerland: World Health Organization; c2020 [cited 2021 Jan 28].
- Paintsil E.COVID-19 threatens health systems in sub-Saharan Africa: the eye of the crocodile. J Clin Invest [Internet]. 2020 Mar 30 [cited 2023 Jul 31];130(6):2741-4. https://doi.org/10.1172/JCI138493 PubMed | Google Scholar
- World Health Organization.International Health Regulations (2005)[Internet]. 2nd ed. Geneva, Switzerland: World Health Organization; 2008 [cited 2023 Jul 31]. 74 p.
- Ministry of Health and Child Care (ZW). Zimbabwe Preparedness and Response Plan: Coronavirus Disease 2019 (Covid-19) [Internet]. Harare, Zimbabwe: Ministry of Health and Child Care; 2020 Mar 19 [cited 2021 Jun 10]. 37 p.
- WHO:Zimbabwe Country Overview [Internet]. Harare, Zimbabwe: World Health Organization; c2023. The current COVID-19 situation; 2003[updated 2023 Aug 2; cited 2021 May 23]; [about 4 screens].
- Zimbabwe National Statistics Agency.Masvingo Province District Population Projections Report [Internet]. Harare, Zimbabwe: ZIMSTAT; 2020 Jun 3 [cited 2023 July 31]. 74 p.
- Phiriyasart F, Chantutanon S, Salaeh F, Roka A, Thepparat T, Kaesaman S, Useng A, Abu I, Weruma R, Arrong S, Sangsawang C.Outbreak investigation of coronavirus disease (COVID-19) among Islamic Missionaries in Southern Thailand, April 2020. OSIR [Internet]. 2020 Jun 30 [cited 2023 Aug 1];13(2):48-54. https://doi.org/10.59096/osir.v13i2.262819 Google Scholar
- Admou B, Hazime R, Brahim I, El Adib AR.Influencing factors of SARS-COV2 spread in Africa.J Glob Health [Internet]. 2020 Aug 11 [cited 2023 Aug 3];10(2): 020331. https://doi.org/10.7189/jogh.10.020331 PubMed | Google Scholar
- World Health Organization.Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations [Internet]. Geneva, Switzerland: World Health Organization: 2020 Mar 29 [updated 2023 Jul 9; cited 2023 Aug 3]. WHO reference number: WHO/2019-nCoV/Sci_Brief/Transmission_modes/2020.2 Google Scholar
- Contini D, Costabile F. Does air pollution influence covid-19 outbreaks? Atmosphere [Internet]. 2020 Apr 13 [cited 2023 Aug 3];11(4):377. https://doi.org/10.3390/atmos11040377
- Zhang S, Wang Z, Chang R, Wang H, Xu C, Yu X, Tsamlag L, Dong Y, Wang H, Cai Y.COVID-19 containment: China provides important lessons for global response . Front Med [Internet]. 2020 Mar 25 [cited 2023 Aug 3];14(2):215-9. https://doi.org/10.1007/s11684-020-0766-9 PubMed | Google Scholar
- García LY, Cerda AA.Contingent assessment of the COVID-19 vaccine . Vaccine [Internet]. 2020 Jul 22 [cited 2023 Aug 3];38(34):5424-9. https://doi.org/10.1016/j.vaccine.2020.06.068 Google Scholar