Preparedness and Perception of Graduates and Trainees of Nigeria Field Epidemiology and Laboratory Training Program towards Participation in COVID-19 Outbreak Response
Azuka Stephen Adeke1,2,&, Chukwuma David Umeokonkwo1,2, Rahab Charles-Amaza1,3, Nkechi Elizabeth Ebere1,2, Hashim Abdulmumin Bala1, Muhammad Shakir Balogun1,4, Patrick Nguku4, Kelly Osezele Elimian3, Chikwe Ihekweazu3
1Nigeria Field Epidemiology and Laboratory Training Program, Abuja, Nigeria, 2Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria, 3Nigeria Center for Disease Control, Abuja, Nigeria, 4African Field Epidemiology Network, Abuja, Nigeria
&Corresponding author
Azuka Stephen Adeke, Department of Community Medicine, Alex Ekwueme Federal University Teaching Hospital Abakaliki, Ebonyi State, Nigeria. azukaadeke@gmail.com
Introduction:
Health workforce is one of the six building blocks of a resilient health system and is key to outbreak control. We assessed preparedness and perception of graduates and trainees of Nigeria Field Epidemiology and Laboratory Training Program (NFELTP) towards participation in COVID-19 response.
Methods:
A cross-sectional study was carried out among 231 respondents. Respondents were graduates and trainees of NFELTP. Electronic self-administered questionnaire was used to collect information from the respondents. We described binary variables using frequencies and percentages; and normally distributed continuous variables using means and standard deviations. Responses to open-ended questions were analyzed in themes.
Results:
Many respondents (68.4%) had undergone at least one training on COVID-19 surveillance (72.2%), infection prevention and control (63.9%), risk communication (38.6%) and sample collection (31.7%). Respondents had previously participated in outbreaks of 27 health-related events especially Lassa fever, poliomyelitis, measles, cholera and yellow fever. Respondents were willing to be engaged in the response (86.6%), despite its novelty, although, 33.8% expressed apprehension for being infected in the course of response to COVID-19 outbreak, while 52.8% mentioned feeling safe in participating in the response.
Conclusion:
NFELTP trainees and graduates should be continuously engaged in outbreak response activities to enhance capacity of Nigerian health workforce.
Introduction

Coronavirus Disease 2019 (COVID-19) is an infectious disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Since its identification and naming, the disease has spread rapidly to many countries and continents, leading to its declaration as a Public Health Emergency of International Concern (PHEIC) by the World Health Organization (WHO) on 30th January 2020 [1-3]. All countries were advised to prepare for containment, including active surveillance, early detection, isolation and case management, contact tracing and prevention of onward transmission of the disease.
The first case of COVID-19 in Nigeria was reported on 28th February 2020, which resulted in the activation of a level 3 multi-sectoral national emergency operation center (EOC); this is the highest level of response in the country for public health emergencies and is led by the Nigeria Centre for Disease Control (NCDC) [
4]. The index case was a 44-year old Italian citizen who was diagnosed in Lagos State [
4].
Following confirmation of COVID-19 cases in Nigeria, NCDC deployed rapid response teams to all affected States [
4]. A vital component of outbreak response and management is the health workforce, which is one of the six building blocks of a health system [
5]. A well-performing health workforce needs to be available, competent, responsive and productive. One of the ways of achieving these and managing a dynamic workforce is through in-service training programs [
5].
Most countries have set up training programs adapted from the United States (U.S.) Centers for Disease Control (CDC)´s Epidemic Intelligence Service (EIS) program in order to strengthen their disease surveillance and global health security [
6]. Nigeria established her Field Epidemiology and Laboratory Training Program (FELTP) with the support of US CDC in 2008 as an advanced in-service training program in field epidemiology, veterinary epidemiology and public health laboratory epidemiology and management [
7]. Since its inception to date, Nigeria FELTP has enrolled 493 health professionals, presently training its eleventh cohort of residents. The field-based training program is designed to equip health professionals for deployment and respond to health-related events across the country. Since 2018, the NCDC is mandated by law to lead the Nigeria FELTP [
8].
Nigeria FELTP graduates and trainees have been involved in outbreak responses since the program was established in 2008 and were especially instrumental in Nigeria´s 2014 Ebola Virus Disease outbreak [
9]. The graduates hold strategic positions and play important functions in the country´s health security agenda at national and sub-national levels with a focus on disease surveillance, prevention and control.
Preparatory activities (coordination, surveillance, laboratory and data management) towards COVID-19 outbreak in Nigeria commenced prior to the confirmation of the first case, and was coordinated by NCDC, with active involvement of Nigeria FELTP graduates and trainees [
10]. A preparedness technical working group set up by NCDC was led by a Nigeria FELTP graduate. Graduates and trainees also conducted surveillance at points of entry and follow-up of passengers of interest. They took part in a readiness tabletop simulation exercise a day before the first case was detected. However, due to the novelty of SARS-CoV-2 and possible fears of the unknown regarding the disease, there was a general concern among healthcare professionals and the populace about participating in the response in the early phase of the pandemic. Thus, we assessed the preparedness and perception of FELTP graduates and trainees in the context of participating in the COVID-19 outbreak response in Nigeria.
Methods

Study design and setting
We conducted a cross-sectional study among graduates and trainees of Nigeria FELTP in May 2020. Although the program has admitted 493 residents in eleven annual cohorts since its inception to date, only cohorts 10 and 11are currently in the training program with 119 residents combined. Each cohort is made up of medical doctors, veterinarians and laboratorians; and runs for 24 months, with 75% field experience and 25% didactic sessions. The field experiences are supervised under the mentorship of experienced epidemiologists [
11].
Sample size determination and sampling technique
We calculated a minimum sample size of 216 using Cochran formula for cross-sectional studies based on an assumed prevalence of perception towards participation in the outbreak response of 50% at 95% confidence interval (CI), 5% precision and correcting for finite population less than 10,000. Sample size was adjusted to 240 after factoring a 10% non-response rate. However, all the trainees and graduates were approached to be part of the study.
Study instrument and data collection
An electronic self-administered questionnaire was used to collect information from the participants. It consisted of four sections: Section A obtained data on the socio-demographic characteristics of the respondents; section B obtained data on the preparedness of respondents; section C obtained information on the perception of respondents towards participation in COVID-19 outbreak response; and section D obtained data on the respondents´ participation in COVID-19 outbreak response for those that have already been engaged. The questionnaire was distributed electronically to all the graduates and trainees from cohorts 1 to 11 due to the movement restriction and in compliance with the social distancing guideline.
Data management
Data were cleaned by checking for consistency and completeness. Data analysis was done with Epi Info version 7.2 and Microsoft Excel 2016. We described binary variables using frequencies and percentages; and normally distributed continuous variables using means and standard deviations. Responses to open-ended questions were analyzed in themes.
Ethical approval
Ethical approval was obtained from the Research and Ethics Committee of Alex Ekwueme Federal University Teaching Hospital Abakaliki with approval number 05/05/2020-27/05/2020. Respondents were informed of their voluntariness to participate in the study, and confidentiality and anonymity of data collected were maintained by avoiding inclusion of possible identifiers, such as names and contact details.
Results
A total of 231 respondents aged between 28 years and 59 years participated in the study with a mean age of 40.4±5.7 years. The highest proportion of the respondents were in the age group of 35-44 years 150 (64.9%). Two-thirds were males 154 (66.7%), 115 (49.8%) were of the medical track of the FELTP, cohorts 9 to 11 constituted 132 (57.1%), and 112 (48.5%) were working primarily in a Federal Government ministry or establishment Table 1.
Most of the respondents 158 (68.4%) had undergone training on COVID-19 with a primary focus on surveillance (114, 72.2%), infection prevention and control (101, 63.9%), risk communication (61, 38.6%) and sample collection (50, 31.7%)
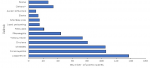
Table 2. Prior to the outbreak, respondents had participated in other outbreaks of 27 diseases and health-related events in Nigeria. A higher proportion of the respondents had been involved in outbreaks of Lassa fever (137, 59.31%), poliomyelitis (106, 45.89%), measles (105, 45.45%), cholera (81, 35.1%) and yellow fever (74, 32.0); whereas, 27 (11.7%) of the respondents had not participated in any response prior to the COVID-19 outbreak
Figure 1.
Many of the respondents (181, 78.4%) expressed readiness and willingness to participate in COVID-19 outbreak response in Nigeria, with the majority acknowledging being current with information on COVID-19 case definition (180, 77.9%) as well as being able to identify some of the common symptoms of COVID-19 including fever (231, 100.0%), shortness of breath (227, 98.3%), cough (226, 97.8%), diarrhea (151, 65.4%) and running nose (140, 60.6%). One hundred and ninety-three (83.6%) of the respondents however acknowledged that COVID-19 patients may be asymptomatic. In a situation where there was a suspected case of COVID-19 infection to be investigated, most of the respondents expressed confidence in being able to handle such a case (169, 73.2%), the use of personal protective equipment (204, 88.3%) and also knew the precautions to take during sample collection from a case (205, 88.7%). Regarding the areas of interest about the outbreak response, more respondents preferred responding under surveillance (140, 60.6%), coordination (37, 16.0%), and risk communication (19, 8.2%)
Table 2.
Concerning the perception of Nigeria FELTP graduates and trainees towards participating in COVID-19 response, more respondents were willing to be engaged in the response (200, 86.6%), and even if the country´s health system got overwhelmed with the outbreak, 198 (85.7%) of them were still willing to participate in the outbreak response. Although, a majority were willing to be part of the response, 78 (33.8%) were apprehensive of being infected with SARS-CoV-2 in the course of responding to the outbreak while 122 (52.8%) had a feeling of being safe in participating in the outbreak response. Fewer respondents were anxious about participating in the response (61, 26.4%) and satisfied with the logistics support provided for engagement in the outbreak response (26, 11.3%). Almost all the respondents (210, 90.9%) were of the opinion that field experience from the response would be beneficial to their career development
Table 3. Possible ways that participating in the response to COVID-19 outbreak could be beneficial to respondents were grouped into the following: 106 respondents believed that they would acquire experience that would improve their capacity for future public health emergencies; 53 were of the views that more knowledge about the disease and its outbreak response would be acquired; 10 said the response could provide them with opportunities for international engagements; 3 regarded the response as an opportunity to carry out research; and two considered the opportunity to network with more public health experts.
One hundred and seventy-five (75.8%) of the respondents had been involved in COVID-19 outbreak response, majority of whom were involved in surveillance (139, 79.4%), coordination (57, 32.6%), infection prevention and control (45, 25.7%), data management (43, 24.6%) and risk communication (37, 21.1%)
Table 4. Some of the recommendations of respondents who had been involved in the outbreak response on ways to improve the response strategies include: improvement of response coordination at both national and state levels; better leadership and political will to enhance resource mobilization for response; reduction of political interference at the operational level of the response by political officials; deployment of more trained field epidemiologists to support the response with their technical skills at the subnational levels; and improvement of logistics support provided for deployment. Other recommendations by the respondents include training of healthcare workers at the local level on aspects of outbreak response, provision of more personal protective equipment to the health workforce, setting up of more laboratories to improve testing capacity and testing turnaround time, more community engagements and risk communication as well as increase in surveillance activities at the local level. Some respondents recommended more collaborations with partners, need to enforce different existing guidelines on COVID-19 as well as more engagement of security personnel to assist the frontline healthcare workers and ensure their safety while working.
Discussion
Capacity building of health professionals is critical to a disease outbreak response, especially for a novel viral disease that has resulted in a pandemic. Equally important to achieving prompt and appropriate responses to an infectious disease outbreak is availability and readiness of trained health professionals. This study has demonstrated that the robust epidemiologic capacity built over the last decade in Nigeria is responsive to national public health priorities. Trained public health personnel have always played critical roles in the control of disease outbreaks [12]. In one of Nigeria´s largest outbreaks of Lassa fever in 2018, FELTP graduates and residents were instrumental in the outbreak response [13]. These group of Nigeria´s public health workforce have also played key roles in preparedness efforts towards yellow fever outbreak in Nigeria [14], as well as its response [15]. In this study, we observed that the respondents were well motivated and eager to participate fully in the different arms of the pandemic response in Nigeria. A high proportion of the respondents had been involved in COVID-19 outbreak response at the time of the study. At the time of commencement of the study, 205 graduates and trainees of the Nigeria FELTP had been deployed to 34 states of the country including the Federal Capital Territory where COVID-19 had been confirmed [16].
We observed that a high proportion of the graduates and trainees were knowledgeable about COVID-19, had undergone training on the disease and are willing to participate in the outbreak response. Similar finding has earlier been reported in the Eastern Mediterranean Region [
17]. The involvement of FELTP graduates has been reported to improve the detection and response to previous similar respiratory pathogens, such as H1N1 virus [
18]. The program has contributed substantially to strengthening public health workforce in Nigeria especially in the areas of public health emergency response and surveillance systems; hence, it is a major public health asset within Nigeria´s national public health institute [
7]. Nigeria FELTP graduates and trainees played a vital role in the containment of the 2014 Ebola Virus Disease outbreak in Nigeria and also supported the disease response in some other West African countries including Sierra Leone and Liberia [
9]. FELTPs have played crucial roles in public health in Africa, and since the declaration of the COVID-19 outbreak as a PHEIC, graduates and trainees of these programs have actively participated in preparedness and response activities within their respective host countries´ Ministries of Health [
19].
Graduates and trainees of the field-based programs in different regions of the world are involved in conducting preparedness assessments, point of entry screening and surveillance of suspected cases, developing protocols and guidelines for surveillance, infection prevention and control, risk communication and community engagement activities in the COVID-19 pandemic [
20,
21]. Being trained to be ready for deployment always, it is not surprising that most of the respondents acknowledged that they were prepared to be deployed for the outbreak response. As observed in this study, most of the FELTP graduates and trainees have participated in major outbreaks in Nigeria like those of Lassa fever, measles, poliomyelitis, yellow fever and cholera. Experiences from previous outbreaks hone the capacity of field epidemiologists. In a study on response capacity of field epidemiology training programs (FETPs) between 2005 and 2016, FETP residents had responded to about 3,300 outbreaks globally and the experience had prepared them to handle problems of national and international concern [
12].
The Training Programs in Epidemiology and Public Health Interventions Network (TEPHINET) desires to develop a strong global workforce that is ready and willing to respond to public health threats [
22]. In this study, many graduates and trainees were willing to participate in the outbreak response even if the outbreak overwhelms the country´s health system, although few of them were anxious about being involved in the response. This is not unexpected, given the novelty of the virus and the fact that many healthcare workers had been infected and died in several countries including Russia, the United Kingdom and the United States of America [
23,
24]. A systematic review of 13 cross-sectional studies involving over 30,000 participants showed that a high proportion of health professionals had experienced significant levels of anxiety, depression and insomnia in the COVID-19 pandemic [
25]. However, almost all the respondents were not satisfied with the logistics provided for deployment in the response. A key component of outbreak preparedness and response is logistics, although, it may be problematic in developing countries. An instance was when FETP graduates deployed to Liberia in 2014 for Ebola Virus Disease outbreak faced logistic challenges in the course of their work [
26]. The need for adequate provisions for logistics cannot be overemphasized, hence the support of governments, partners, and private donors is key to ensuring logistics support are adequate for response to outbreaks.
A limitation in this study is the possibility of response bias as majority of the respondents have been involved in COVID-19 response; hence responses by respondents with prior experience from COVID-19 response might be systematically different from those without any experience.
Conclusion
The graduates and trainees of the Nigeria FELTP have demonstrated good preparedness, experiential capacity and willingness to fully participate in the COVID-19 outbreak response. The result from this study and earlier studies demonstrated that these graduates and trainees are useful in surveillance, early detection, and mounting appropriate innovative response to the disease threats across different regions. We recommend that they are continuously engaged in outbreak response activities at different levels as they contribute to enhancing the capacity of the health workforce in the country.
What is known about this topic
- Health workforce is one of the six building blocks of a resilient health system and is key to outbreak control
- One of the ways of achieving and managing a dynamic workforce is through in-service training programs
What this study adds
- The graduates and trainees of the Nigeria FELTP have demonstrated good preparedness, experiential capacity and willingness to fully participate in the COVID-19 outbreak response
- These graduates and trainees are useful in surveillance, early detection, and mounting appropriate innovative response to the disease threats across different regions of Nigeria
Competing interests
The authors declare no competing interests.
Authors' contributions
Azuka Stephen Adeke conceptualized and designed the study, implemented data acquisition and analysis, and drafted the initial manuscript. Chukwuma David Umeokonkwo designed the study, implemented data acquisition and analysis, and made substantial revision of initial manuscript. Rahab Charles-Amaza, Nkechi Elizabeth Ebere, Hashim Abdulmumin Bala, and Muhammad Shakir Balogun designed the study, implemented data acquisition, and made substantial revision of initial manuscript. Patrick Nguku, Kelly Osezele Elimian, and Chikwe Ihekweazu made substantial revision of initial manuscript. All authors have read and approved the final version.
Tables and figures
Table 1: Socio-demographic characteristics of respondents
Table 2: Preparedness of Nigeria FELTP graduates and residents towards participation in COVID-19 outbreak response in Nigeria
Table 3: Perception of Nigeria FELTP graduates and residents towards participation in COVID-19 outbreak response in Nigeria
Table 4: Participation of NFELTP graduates and residents in COVID-19 outbreak response
Figure 1: Participation of respondents in previous outbreaks of health-related events (Others﹡- these included outbreak of snakebite, mumps, rabies, unknown illness, swine flu, methanol poisoning, food poisoning, chlorine poisoning, rubella, necrotizing enterocolitis, chicken pox, tetanus, diphtheria, dengue fever, hepatitis B, and scabies)
References
- World Health Organization. Q&A on coronaviruses (COVID-19). WHO. 2020 Accessed July 2020.
- World Health Organization. Rolling updates on coronavirus disease (COVID-19). WHO. 2020. Accssed July 2020.
- World Health Organization. Novel Coronavirus - China. WHO. 2020. Accssed July 2020.
- Nigeria Centre for Disease Control. An update of COVID-19 outbreak in Nigeria. NCDC. 2020. Accessed July 2020.
- World Health Organization. Everybody´s business: Strengthening health systems to improve health outcomes: WHO´s framework for action. Geneva, WHO. 2007. Accessed July 2020.
- Schneider D, Evering-Watley M, Walke H, Bloland PB. Training the Global Public Health Workforce Through Applied Epidemiology Training Programs: CDC´s Experience, 1951-2011. Public Health Rev. 2011; 33(1):190-203. Google Scholar
- Nguku P, Oyemakinde A, Sabitu K, Olayinka A, Ajayi I, Fawole O, Babirye R, Gitta S, Mukanga D, Waziri N, Gidado S, Biya O, Gana C, Ajumobi O, Abubakar A, Sani-Gwarzo N, Ngobua S, Oleribe O, Poggensee G, Nsubuga P, Nyager J, Nasidi A. Training and service in public health, Nigeria Field Epidemiology and Laboratory Training, 2008 - 2014. Pan Afr Med J. 2014; 18(Suppl 1):2.https://doi.org/10.11694/pamj.supp.2014.18.1.4930 . PubMed | Google Scholar
- NCDC. Nigeria Centre for Disease Control and Prevention (Establishment) Act 2018. NCDC. 201 Accessed July 2020.
- Training Programs in Epidemiology and Public Health Interventions Network. Nigeria Field Epidemiology and Laboratory Training Program. TEPHINET. Accessed July 2020.
- Training Programs in Epidemiology and Public Health Interventions Network. FETP Activities in Response to Coronavirus Disease 19 (COVID-19). TEPHINET. 2020. Accessed July 2020.
- Nguku PM, Umeokonkwo CD, Balogun MS, Waziri NE, Bashorun AT, Ntadom G, Ihekweazu C. Sharing Experiences from the Field: updates from the Nigeria Field Epidemiology and Laboratory Training Program. Pan Afr Med J. 2019; 32(Suppl 1):1.https://doi.org/10.11604/pamj.supp.2019.32.1.18136 . PubMed | Google Scholar
- Jones DS, Dicker RC, Fontaine RE, Boore AL, Omolo JO, Ashgar RJ, Baggett HC. Building global epidemiology and response capacity with field epidemiology training programs. Emerg Infect Dis. 2017; 23(December):S158-65.https://doi.org/10.3201/eid2313.170509 . PubMed | Google Scholar
- World Health Organization. Lassa fever - Nigeria. WHO. 2018. Accessed July 2020.
- Okunromade OF, Lokossou VK, Anya I, Dada AO, Njidda AM, Disu YO, Dalhat MM, Brito CF De, Balogun MS, Nguku P, Ojo OE, Ihekweazu C, Okolo S. Performance of the Public Health System during a Full-Scale Yellow Fever Simulation Exercise in Lagos State, Nigeria, in 2018: How Prepared Are We for the Next Outbreak. Heal Secur. 2019; 17(6):485-94.https://doi.org/10.1089/hs.2019.0048 . Google Scholar
- African Field Epidemiology Network. Nigeria FELTP Conduct Yellow Fever Outbreak Investigation in Anambra State. AFENET. 2019. Accessed July 2020.
- African Field Epidemiology Network. 205 residents and graduates of the Nigeria FELTP deployed on COVID-19 Response to 34 States. AFENET. 2020. Accessed July 2020.
- Al Nsour M, Khader Y, Al Serouri A, Bashier H, Osman S. Awareness and Preparedness of Field Epidemiology Training Program Graduates to Respond to COVID-19 in the Eastern Mediterranean Region: Cross-Section Study. JMIR Med Educ. 2020; 6(2):e19047.https://doi.org/10.2196/19047 . PubMed | Google Scholar
- Idubor OI, Kobayashi M, Ndegwa L, Okeyo M, Galgalo T, Kalani R, Githii S, Hunsperger E, Balajee A, Verani JR, da Gloria Carvalho M, Winchell J, Van Beneden CA, Widdowson M-A, Makayotto L, Chaves SS. Improving Detection and Response to Respiratory Events – Kenya, April 2016-April 2020. MMWR Morb Mortal Wkly Rep. 2020 May; 69(18):540-4.https://doi.org/10.15585/mmwr.mm6918a2 . PubMed | Google Scholar
- African Field Epidemiology Network. Coronavirus disease 2019 (COVID-19) Preparedness in Africa: The Role of African Field Epidemiology and Laboratory Training Programs (FELTPs). AFENET. 2020. Accessed July 2020.
- Al Nsour M, Bashier H, Al Serouri A, Malik E, Khader Y, Saeed K, Ikram A, Abdalla AM, Belalia A, Assarag B, Baig MA, Almudarra S, Arqoub1 K, Osman S, Abu-Khader I, Shalabi D, Majeed Y. The role of the global health development/eastern mediterranean public health network and the eastern mediterranean field epidemiology training programs in preparedness for COVID-19. JMIR Public Health Surveill. 2020; 6(1):e18503.https://doi.org/10.2196/18503 . PubMed | Google Scholar
- African Field Epidemiology Network. COVID-19 How prepared is the African Continent. AFENET. 2020. Accessed July 2020.
- Training Programs in Epidemiology and Public Health Interventions Network. 20th Anniversay Report: Training Programs in Epidemiology and Public Health Interventions Network. TEPHINET. 2018. Accessed July 2020.
- Chalmers V. UK has recorded more Covid-19 deaths among healthcare workers than ANY country in the world except Russia, report reveals. Mail Online. 2020. Accessed July 2020.
- Babb K, Shammas B, Cha EA. Hundreds of health-care workers lost their lives battling the coronavirus. The Washington Post. 2020. Accessed July 2020.
- Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun. 2020; 88: 901-907.https://doi.org/10.1016/j.bbi.2020.05.026 . PubMed | Google Scholar
- Lubogo M, Donewell B, Godbless L, Shabani S, Maeda J, Temba H, Malibiche TC, Berhanu N. Ebola virus disease outbreak; the role of field epidemiology training programme in the fight against the epidemic, Liberia, 2014. Pan Afr Med J. 2015;22(Supp 1):5.https://doi.org/10.11694/pamj.supp.2015.22.1.6053 . PubMed | Google Scholar