Prevalence and factors associated with unintended pregnancies in teenagers and young women in eight Sub-Saharan African countries: evidence from Performance Monitoring and Accountability cross-sectional surveys, (2017-2018)
Dobo Onivogui1,&, Abou Coulibaly1,2, Desire Lucien Dahourou2,3, Seni Kouanda1,2
1Institut Africain de Santé Publique (IASP), Ouagadougou, Burkina Faso, 2Institut de Recherche en Sciences de la Santé (IRSS), Ouagadougou, Burkina Faso, 3Centre International Recherche en Santé de Ouagadougou, Burkina Faso
&Corresponding author
Dobo Onivogui, Institut Africain de Santé Publique (IASP), Ouagadougou, Burkina Faso.
Introduction:
Sub-Saharan Africa is one of the world's regions with a low modern contraceptive prevalence rate and a high prevalence of unintended pregnancies. This study aimed to explore the prevalence and contributing factors to unintended pregnancies among teenagers and young women in eight sub-Saharan African countries.
Methods:
We analyzed Performance Monitoring and Accountability 2020 (PMA 2020) data from eight countries in sub-Saharan Africa (Ghana, Burkina Faso, Niger, Côte d'Ivoire, Nigeria, Uganda, Ethiopia, and Kenya) that had conducted the national surveys in 2017-2018. A total of 4,914 young women aged 15 to 24 years who were pregnant at the time of data collection or who had given birth between 2016 and 2018 were involved in this study. We determined the pooled prevalence, and by country, of unintended pregnancies. We used binary logistic regression to explore the factors associated with unintended pregnancies.
Results:
The pooled prevalence of unintended pregnancies for all eight countries was 33.4% (95% CI =31.0 - 36.0), ranging from 13.0% (6.8 -15.1) in Niger to 55.8% (46.9 - 64.8) in Ghana. Educated women, never-married women, and women who had unmet needs for contraception were more likely to have unintended pregnancies. In contrast, women with moderately rich, rich, and very rich profiles are less likely to have unintended pregnancies.
Conclusion:
Despite the efforts made, the prevalence of unintended pregnancies is still high in seven countries, except Niger. Reducing unmet needs remains the priority for the prevention of unintended pregnancies.
Introduction

Unintended pregnancies are an important public health problem in sub-Saharan African countries because of their associations with induced abortions and numerous obstetric complications [1-4]. Between 2010 and 2014, there was a worldwide rate of 62 (59-72) unintended pregnancies per 1000 women aged 15-44 per year. Of these unintended pregnancies, 56% resulted in abortions [4]. According to the World Health Organization (WHO), 4.7% to 13.2% of maternal deaths are recorded each year worldwide due to unsafe abortions, most of which follow unintended pregnancies [5].
Sub-Saharan Africa has a significant proportion of unintended pregnancies. From 2010 to 2014, the unintended pregnancies prevalence was 85 per 1000 women in the age group 15-44 years. The highest rate was observed in East Africa, with 112 unintended pregnancies per 1000 women aged 15 to 44 years [
4].
All women of childbearing potential may be affected by unintended pregnancies. But adolescent girls aged 15 to 19 years and young women aged 20 to 24 years suffer more of the consequences, including exclusion from the parental family, dropping out of school, induced abortions, or maternal and neonatal deaths [
1,
6,
7].
Adolescent girls are exposed to occasional sexual practices without any experience of using contraceptive methods with risks of pregnancy and sexually transmitted infections [
8]. In some communities where pronatalist norms are pervasive, young women are confronted with social norms that would like the woman to prove her fertility from the moment of marriage to benefit from a particular social consideration. Thus, from the first year of marriage, women are subjected to cultural and religious pressures that expose them to unintended pregnancies [
8,
9].
Several factors can explain the occurrence of unintended pregnancy in adolescents and young women. These factors include early marriage, pronatalist cultures, rural residence, religion, low social and economic support for girls, curiosity, peer pressure, lack of comprehensive sexuality education and unmet need for contraceptive methods [
10,
11]. However, the main risk factor is the non-use or inefficient use of contraceptive methods [
10,
11].
To respond to the low use of contraceptive methods, many actions have been tried worldwide, including the “Family Planning 2020” (FP2020) initiative, born from the 2012 London International Summit on Family Planning. The countries participating in this summit committed themselves to ensuring that by 2020, an additional 120 million women in developing countries would have free access to modern contraceptive methods [
12]. After this summit, several studies were conducted on teenage pregnancies in general [
6,
13-15]. However, there are very few studies that focus mainly on unintended pregnancies in adolescent girls and young women at the national or sub-national level [
15-18]. Previous studies on several countries used data from surveys carried out at periods with almost ten-year differences. So, this study aimed to estimate the prevalence of unintended pregnancies in teenagers in several sub-Saharan African countries using data from the 2017 and 2018 surveys and determining the associated factors.
Methods

Study settings
The PMA2020 project concerns eleven priority countries, including nine in sub-Saharan Africa, where the surveys are conducted. In Africa, surveys are carried out in Ghana, Burkina Faso, Niger, Côte d'Ivoire, Nigeria, the Democratic Republic of The Congo (DRC), Uganda, Ethiopia, and Kenya. In this study, we analyzed data from eight countries that had organized the national surveys in 2017-2018 (
Figure 1). DRC was omitted because the surveys are restricted to one province.
Data sources
Performance Monitoring and Accountability 2020 (PMA2020) was created to provide rapid and frequent estimates of modern contraceptive use in FP2020 priority countries. PMA2020 conducts surveys every six months to one year, providing FP2020, governments, and other stakeholders frequent information on contraceptive use, demand, and supply that can inform policies and programs and identify areas for improvement [
19]. PMA2020 microdata are accessible on request through the project website (
http://www.pma2020.org/request-access-to-datasets-new ) upon approval by PMA2020's coordinating center. We downloaded separate datasets for each country. All the databases for the eight countries were combined into a single database, on which we performed the analysis.
Study type and population selection criteria
This is a secondary analysis of PMA2020 data. The PMA2020 surveys are repeated cross-sectional surveys based on a multistage stratified cluster sampling design, and the primary sampling units or enumeration areas are selected by probability proportional-to-size method for which the sample selection probability depends on the size of population. Further details on PMA methodology are available online [
19,
20].
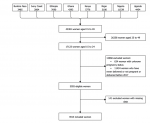
This analysis involved women aged 15 to 24 years who were pregnant at the time of data collection or who had given birth between 2016 and 2018. Thus, we excluded women who gave birth before 2016, those whose pregnancy status is unknown, those who were never pregnant, and those with missing data (
Figure 2).
Sample description
The surveys involved 43,381 women of childbearing age (15 to 49 years). Of these women, 17,123 (39.5%) were between 15 and 24 years. Based on our inclusion criteria, 4,914 women aged 15 to 24 years were pregnant or had given birth at the time of the various surveys.
Figure 2 describes the sample selection process for analysis.
Table 1 describes the distribution by country and by variables of the adolescent girls and young women in our study.
Study variables
Dependent variable: an unintended pregnancy is defined as a pregnancy that occurs in a concept without the partners having planned to have it. It may happen when no child is wanted, or it may be untimely (that is, it occurred earlier than expected). It can occur following consensual or non-consensual sexual intercourse (including rape), apart from using a contraceptive method. However, some unintended pregnancies are secondary to contraceptive failure [
21,
22 ]. PMA in cross-sectional and panel surveys asked the woman about the intentionality of her last birth or current pregnancy. This indicator is based on responses to the question, “At the time you became pregnant, did you want to become pregnant then, did you want to wait until later, or did you not want to have any/any more children at all?” It is measured as the percent of women of childbearing age reporting their most recent or current pregnancy was wanted then, wanted later, or not wanted at all. So, the dependent variable was defined by using this variable. Given the small number in the “not wanted at all” modality, we added it to the number of the “Later” modality to constitute the unintended pregnancy modality (coded 1 for yes). Thus, the pregnancy was intended if the woman responded that it was wanted (coded 0 for no). Thus, the dependent variable was binary (0=wanted pregnancy, 1=unintended pregnancy).
Independent variables: The selection of the independent variables was guided by the literature review and the availability of variables in the database. The selected independent variables were (i) the woman's sociodemographic characteristics (country, wealth quintile, age, level of education, marital status, residence) (ii) family planning indicators (unmet need, home visit by a health worker to discuss FP in the last 12 months, information about FP through the media), and (iii) woman´s age at first sexual intercourse. For the assessment of household wealth, some countries use quintiles, while others use wealth tertiles. For compliance, we calculated the level of wealth in five categories for all bases with wealth tertiles using the score variable, which was calculated by principal component analysis (PCA).
Data analysis
Data analyses were done using Stata version 15.0 [
23], and for statistical significance, the considered alpha (type-I error) is 0.05. Firstly, we described the participants´ characteristics. Second, we determined the pooled weighted prevalence of unintended pregnancies, as well as the weighted prevalences by country and for all categories of the selected independent variables. We used binary logistic regressions to evaluate the association between the independent and dependent variables. All variables with a significance of less than 0.20 (i.e., with a p-value < 0.20) during the bivariate analysis were included in the multivariate model [
24]. We used the forward selection method of variable selection by starting with no variables in the model and then adding other variables to the model one by one until any variable not included in the model could significantly contribute to our outcome. Successive models were compared using the likelihood ratio test. The binary logistic regression analysis results were presented as odds ratio (OR) with corresponding 95% confidence intervals and p-values. Previous studies have guided the choice of methods of reference for the variables [
3,
6,
24]. For the country of residence, the choice of Ethiopia as the reference country was based on studies that show that this country is an excellent example of FP in the sub-Saharan Africa [
25,
26]. The use of a multivariate model therefore allowed us to control for potential confounding factors.
Multi-collinearity between independent variables was verified using variance inflation factors (VIF). The Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were used to choose the model that best explains the dependent variable, so during the comparison, the model with the lowest AIC was chosen. The quality of the overall fit of the final model was verified using the Hosmer-Lemeshow test when the probability of chi2 is more significant than 0.05, which indicates that the model is well adjusted. The discriminating power of the model was verified through the area under the curve ROC (receiver operating characteristic) [
27].
Ethical considerations
We used secondary data that the various countries' ethics committees had approved prior to the data collection [
28]. PMA surveys have also been conducted after obtaining ethical approval from Bloomberg School of Public Health at Johns Hopkins University in Baltimore, USA [
29]. We requested data from the PMA2020 management program (Performance Monitoring and Accountability 2020). The data was used according to ethical guidelines and data protection regulations. In each country, the data contained no information that could formally identify a woman.
Results
Prevalence of unintended pregnancies
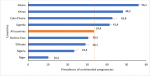
The pooled prevalence of unintended pregnancies was 33.4% (95% CI =31.0 - 36.0). We found a significant disparity in the prevalence of unintended pregnancies between the eight countries (
Figure 3). By country, the highest prevalence was observed in Ghana with 55.8% (95% CI = 46.9 - 64.8), followed by Kenya with 45.7% (95% CI = 42.6 - 53.9). The lowest prevalence of unintended pregnancies is observed in Niger (13.0 %) (95% CI = 6.8 -15.1).
Predictors of unintended pregnancies in adolescent girls and young women
In the multivariate analysis (
Table 2), Kenyan women had a statistically significantly higher probability of unintended pregnancy than women from Ethiopia (aOR: 1.8; 95% CI: 1.2 - 2.8). On the other hand, the probability of unintended pregnancy was statistically significantly lower for women who resided in Niger (aOR: 0.3; 95% CI: 0.1 - 0.4) and Nigeria (aOR: 0.4; 95% CI: 0.2 - 0.6). Comparing women from other countries with those from Ethiopia showed no significant difference.
Compared to those who were not educated, educated women (primary, secondary, or higher) were more likely to have unintended pregnancies. Common-law/cohabiting women were significantly more likely to have unintended pregnancies than married women with (aOR:1.7; 95% CI 1.2-2.3) and so were the divorced, widowed or never-married women (aOR: 7.3; 95% CI 5.5-9.8). Women in wealthy quintiles (middle, wealthier, and wealthiest) were significantly less likely to have unintended pregnancies than women in the poorest wealth quintiles with (aOR: 0.7; 95% CI 0.5-0.9), (aOR: 0.7; 95% CI 0.4-0.9) and (aOR: 0.7; 95% CI 0.5-0.9) respectively. Women who had unmet family planning needs were about 13 times more likely to have unintended pregnancies than women whose FP needs were met (aOR:12.7; 95%CI 10.2-15.9).
Discussion
Prevalence of unintended pregnancies among adolescent girls and young women
Our study shows a disparity in the prevalence of unintended pregnancies among teenagers and young women between countries. While the prevalence is high in some countries, it is low in others. Reproductive health policies and sociocultural norms could explain these differences among countries. This low prevalence of unwanted pregnancies can also be explained by women's strong desire for fertility in certain countries. For instance, a study by Chukwudeh and Oduaran showed that parental pressure, the desire for more children, the desire for male children, values placed on children, norms, and pronatalist culture were associated with high fertility in sub-Saharan Africa [
30]. So, given the pronatalist cultures prevalent in those settings, which often condition women to want children and see every pregnancy as intended, wanted, desired and welcomed, they could accept all pregnancies. Previous studies found that Niger had the lowest rate of unintended pregnancy, such as a study comparing 166 countries around the world [
31]. Another study showed that the desire for fertility among women of childbearing age was 97.2% in Niger, based on data from the 2012 Demographic and Health Surveys (DHS) data with even more pronounced fertility desire among young women [
32]. Another reason that could explain the unintended pregnancy prevalence disparity is the high prevalence of child marriage: a study in 11 West African countries with DHS data revealed that this prevalence was 41.5% [
33]. Lastly, we think some level of knowledge and agency are required for women to be able to consider a pregnancy as unintended. This condition, in our opinion, revealed the limitation of unintended pregnancy as an indicator or marker of reproductive health, making it as a subjective construct because women need some degree of autonomy, agency and awareness on family planning to be able to consider their pregnancy unintended this, coupled with pro-natalist norms, was what accounted for the low prevalence of unintended pregnancies in Niger and, to a lesser extent, in Nigeria. Another result to consider is the relatively high prevalence of unintended pregnancies in Ethiopia, despite being cited as one of the good examples of family planning in sub-Saharan Africa [
25,
26].
Factors associated with unintended pregnancies
Our results show that high levels of education are not a protective factor in unintended pregnancies. Therefore, the higher the educational attainment of adolescent girls and young women, the more likely they will have unintended pregnancies. This result is similar to that of a study conducted in the DRC [
34] and contrary to several other studies [
21,
35,
36 ]. This could be because young women are familiar with contraceptive methods through awareness sessions, but because they fear side effects, they prefer to abstain from their uses. In addition, they are still young and are mostly either in school or in the apprenticeship phase of trade; they maintain sexual relations for reasons other than reproductive needs. Thus, a pregnancy in these situations is likely to be unintended.
Adolescent girls and young women from wealthy households were less likely to have unintended pregnancies. This study aligns with those of Wado et al., conducted in five East African countries and Dixit in India [
37,
38]. The precarious socioeconomic status of parents makes adolescent girls vulnerable to pregnancy. To meet their basic needs, adolescent girls engage in relationships. Such relationships with economic dependence make the girl powerless to impose on her partner the use of condoms. On the other hand, girls from wealthier families already have their needs covered by their families. As a result, they may be afraid of getting pregnant and at risk of being rejected by the family.
The study found that women in union but without formal marriage were likely to report unintended pregnancies. Divorced, widowed, or never-married women were 7.3. times more likely to report unintended pregnancies than married women. This result is lower than that of Yenealem F. in Ethiopia, who found that single women were 12.59 times more likely to report an unintended pregnancy than married women [
39]. From the perception of some communities, the young married woman still needs to prove her fertility power to be accepted by the in-laws. Even if a pregnancy occurs, these women are less likely to report it for fear of being rejected from the home [
7] or because many cultures in Africa abhor children out of wedlock. For instance, in Burkina Faso, a study report by Zongo et al., in terms of the management of pregnancy before marriage, noted that among the Mossi ethnic group, there were still cases of punishment like being “out-casted” by the family [
40].
We found a strong association between unmet needs and unintended pregnancies. Women with unmet needs for family planning were 12.7 times more likely to have unintended pregnancies than those with met needs. The unmet need for family planning is one of the most important predictors of unintended pregnancies. Our results are consistent with that of Samuel H. Nyarko, who found a significant association between unmet contraceptive needs and unintended pregnancies among pregnant women in Ghana [
9].
This study found no association between media exposure and unintended pregnancies in adolescent girls and young women. Unlike our study, exposure to mass media is considered a protective factor against unintended pregnancies in women in several previous studies [
35,
37,
41]. The nature of the sources of information could explain our findings. With the advent of the internet and smartphones, perhaps the sources of information for young women have changed. When we now know that there is enough false information on social networks, adolescent girls and young women could be exposed to incorrect information related to the side effects of contraceptive methods [
42].
Strength and limitations
First, this study involved many countries with a high fecundity rate. Moreover, the countries´ samples are strong. Hence, our research has good statistical powers that vary between 84% for Burkina Faso, 90% for Ethiopia, and 100% for Côte d'Ivoire, Ghana, Kenya, Niger, Nigeria, Uganda, and the quality of the results of the analyses. However, because PMA2020 was designed to assess contraception use, some variables that would better explain unintended pregnancies had missing values, such as the partner's involvement in contraception use, the intention of using contraceptive methods in the future, and the parity of the woman. These variables were not available for the analysis.
Conclusion
This study showed that the prevalence of unintended pregnancies among young women aged 15 to 24 years is still high in some sub-Saharan African countries. Although national family planning programs made enormous efforts after the London Summit in 2012, unintended pregnancies remain a public health problem.
Based on the results of our study, there are still factors contributing to the occurrence of unintended pregnancies. Among these factors, unmet needs appear to be the most critical factor in unintended pregnancies in the studied countries. Therefore, family planning programs in different countries need to redouble their efforts to reduce this indicator, particularly focusing on the sexual and reproductive health of adolescent girls and young women. The non-contribution of awareness through the media on preventing unintended pregnancies among adolescents and young women is a sign of great concern. With the advent of new information technologies, family planning services should adapt to the communication channels most young people use.
What is known about this topic
- Unintended pregnancies in teenagers and young women are a public health problem in the sub-Saharan region because it often leads to induced abortion and subsequent complications
- The rate of unintended pregnancy is high in sub-Saharan Africa
- The non-use of modern contraceptive methods, coupled with some sociodemographic factors is a significant determinant of unintended pregnancy
What this study adds
- This study reported a high prevalence of unintended pregnancies among adolescents and young women in eight Sub-Saharan African countries
- This prevalence varies across countries
- There are still residual factors among which unmet need plays an essential role in unintended pregnancies among adolescents and young women
Competing interests
The authors declare no competing interests.
Authors´ contributions
DO and AC were involved in the design and conception of the study. DO and AC analyzed and interpreted the data. DO wrote the first draft, and AC, LDD, and SK made substantial corrections. All authors reviewed and approved the final version of the manuscript.
Acknowledgements
The authors thank the database administrators of the performance monitoring and Accountability/2020 (PMA2020) project for making available the databases of the eight countries that are the subject of this study.
Table and figures
Table 1: Distribution of adolescent girls and young women by country and by variable, 2017-2018
Table 2: Univariate and Multivariate analyses of factors associated with unintended pregnancies among adolescent and young women in eight countries in sub-Saharan Africa, 2017-2018
Figure 1: PMA countries involved in the study
Figure 2: Flow diagram of study participants
Figure 3: Prevalence of unintended pregnancies by country among adolescent girls and young women, 2017-2018
References
- Shah IH, Åhman E. Unsafe abortion differentials in 2008 by age and developing country region: high burden among young women . Reprod Health Matters [Internet]. 2012 Jul 9 [cited Oct 21];20(39):169-73. https://doi.org/10.1016/s0968-8080(12)39598-0 Google Scholar
- Chae S, Desai S, Crowell M, Sedgh G. Reasons why women have induced abortions: a synthesis of findings from 14 countries . Contraception [Internet]. 2017 Jul 7 [cited 2024 Oct 31];96(4):233-41. https://doi.org/10.1016/j.contraception.2017.06.014 Google Scholar
- Ameyaw EK, Budu E, Sambah F, Baatiema L, Appiah F, Seidu AA, Ahinkorah BO. Prevalence and determinants of unintended pregnancy in sub-Saharan Africa: A multi-country analysis of demographic and health surveys . PloS ONE [Internet]. 2019 Aug 9 [cited 2024 Oct 21];14(8):e0220970. https://doi.org/10.1371/journal.pone.0220970 PubMed | Google Scholar
- Bearak J, Popinchalk A, Alkema L, Sedgh G.Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical model . Lancet Glob Health [Internet]. 2018 March 5[cited 2024 Oct 21];6(4): e380-9. https://doi.org/10.1016/s2214-109x(18)30029-9 Google Scholar
- Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J, Gülmezoglu AM, Temmerman M, Alkema L.Global causes of maternal death: a WHO systematic analysis . Lancet Glob Health [Internet]. 2014 May 5[cited 2024 Oct 21];2(6):e323-33. https://doi.org/10.1016/s2214-109x(14)70227-x Google Scholar
- Birhanu BE, Kebede DL, Kahsay AB, Belachew AB.Predictors of teenage pregnancy in Ethiopia: a multilevel analysis . BMC Public Health [Internet]. 2019 May 17[ cited 2024 Oct 21];19(1):601. https://doi.org/10.1186/s12889-019-6845-7 PubMed | Google Scholar
- Salami KK, Ayegboyin M, Adedeji IA.Unmet social needs and teenage pregnancy in Ogbomosho, South-western Nigeria . Afr Health Sci [Internet]. 2015 Jan 16 [cited 2024 Oct 21];14(4):959-66. https://doi.org/10.4314/ahs.v14i4.27 Download ajol-file-journals_45_articles_111414_submission_proof_111414-529-308073-1-10-20150116.pdf. PubMed | Google Scholar
- Hindin MJ, Kalamar AM, Thompson TA, Upadhyay UD. Interventions to Prevent Unintended and Repeat Pregnancy Among Young People in Low- and Middle-Income Countries: A Systematic Review of the Published and Gray Literature . J Adolesc Health [Internet]. 2016 Sep [cited 2024 Oct 30];59(3 Suppl):S8-15. https://doi.org/10.1016/j.jadohealth.2016.04.021 Google Scholar
- Dingeta T, Oljira L, Worku A, Berhane Y.Unmet Need for Contraception Among Young Married Women in Eastern Ethiopia . Open Access J Contracept [Internet]. 2019 Dec 17[cited 2024 Oct 21]; 10:89-101. https://doi.org/10.2147/OAJC.S227260 PubMed | Google Scholar
- Yaya S, Ghose B.Prevalence of unmet need for contraception and its association with unwanted pregnancy among married women in Angola . Navaneetham K, editor. PLoS ONE [Internet]. 2018 Dec 31 [cited 2024 Oct 30];13(12):e0209801. https://doi.org/10.1371/journal.pone.0209801 PubMed | Google Scholar
- Berrewaerts J, Noirhomme-Renard F. Les grossesses à l´adolescence: quels sont les facteurs explicatifs identifiés dans la littérature? [ Teenage pregnancies: what explanatory factors have been identified in the literature?][Internet]. Brussels (BE): UCL-RESO; 2006 Jun [cited 2024 Oct 30]. 41 p. (Technical File Series). French. Réf.: 06-40. Community Health Promotion Service with the support of the French Community of Belgium. Full text available on request.
- Ahmed S, Choi Y, Rimon JG, Alzouma S, Gichangi P, Guiella G, Kayembe P, Kibira SP, Makumbi F, OlaOlorun F, Omoluabi E, Otupiri E, Oumarou S, Seme A, Shiferaw S, Anglewicz P, Radloff S, Tsui A. Trends in contraceptive prevalence rates in sub-Saharan Africa since the 2012 London Summit on Family Planning: results from repeated cross-sectional surveys. The Lancet Global Health [Internet]. 2019 May 17 [cited 2024 Oct 30];7(7):e904-11. https://doi.org/10.1016/s2214-109x(19)30200-1 Google Scholar
- Mekonnen Y, Telake DS, Wolde E. Adolescent childbearing trends and sub-national variations in Ethiopia: a pooled analysis of data from six surveys. BMC Pregnancy Childbirth [Internet]. 2018 Jul 3 [cited 2024 Oct 30];18(1):276. https://doi.org/10.1186/s12884-018-1917-8 PubMed | Google Scholar
- Yakubu I, Salisu WJ. Determinants of adolescent pregnancy in sub-Saharan Africa: a systematic review . Reprod Health [Internet]. 2018 Jan 27 [cited 2024 Oct 30];15(1):15. https://doi.org/10.1186/s12978-018-0460-4 PubMed | Google Scholar
- Krugu JK, Mevissen FEF, Prinsen A, Ruiter RAC. Who´s that girl? A qualitative analysis of adolescent girls´ views on factors associated with teenage pregnancies in Bolgatanga, Ghana. Reprod Health [Internet]. 2016 Apr 14 [cited 2024 Oct 30];13(1):39. https://doi.org/10.1186/s12978-016-0161-9 PubMed | Google Scholar
- Izugbara C. Socio-demographic risk factors for unintended pregnancy among unmarried adolescent Nigerian girls . South Afr Fam Pract [Internet]. 2015 Feb 25 [cited 2024 Oct 21];57(2):121-5. https://doi.org/10.1080/20786190.2014.977042 Google Scholar
- Ikamari L, Izugbara C, Ochako R. Prevalence and determinants of unintended pregnancy among women in Nairobi, Kenya. BMC Pregnancy Childbirth [Internet]. 2013 Mar 19 [cited 2024 Oct 21]; 13(1):69. https://doi.org/10.1186/1471-2393-13-69 PubMed | Google Scholar
- Nyarko SH. Unintended Pregnancy among Pregnant Women in Ghana: Prevalence and Predictors . J Pregnancy [Internet]. 2019 Jan 30 [ cited 2024 Oct 21];2019 (1): 920491. https://doi.org/10.1155/2019/2920491 PubMed | Google Scholar
- Zimmerman L, Olson H, Tsui A, Radloff S. PMA2020: Rapid Turn–Around Survey Data to Monitor Family Planning Service and Practice in Ten Countries . Stud Fam Plann [Internet]. 2017 Aug 28 [cited 2024 Oct 21];48(3):293-303. https://doi.org/10.1111/sifp.12031 PubMed | Google Scholar
- Zimmerman L, OlaOlorun F, Radloff S. Accelerating and improving survey implementation with mobile technology: Lessons from PMA2020 implementation in Lagos, Nigeria . Afr Popul Stud [Internet]. 2015 Jun 4 [cited 2024 Oct 21];29(1 Suppl MobTech MNCH):1699-712. https://doi.org/10.11564/29-1-719 Download pdf to view full text. Google Scholar
- Goshu YA, Yitayew AE. Prevalence and determinant factors of unintended pregnancy among pregnant women attending antenatal clinics of Addis Zemen hospital. PLoS ONE [Internet]. 2019 Jan 30 [cited 2024 Oct 27];14(1):e0210206. https://doi.org/10.1371/journal.pone.0210206 PubMed | Google Scholar
- Santelli J, Rochat R, Hatfield K. The Measurement and Meaning of Unintended Pregnancy. Perspect Sex Reprod Health [Internet]. 2007 Feb 12 [cited 2024 Oct 21]; 35(2):94-101. https://doi.org/10.1363/3509403 Download pdf to view full text. Google Scholar
- StataCorp. Stata Statistical Software: Release 15 [software]. 2017 [cited 2024 Nov 11]. Purchase required to access.
- El Sanharawi M, Naudet F. [Understanding logistic regression] . Journal Fr Ophtamol [Internet]. 2013 Aug 14 [cited 2024 Oct 27];36(8):710-5. French. https://doi.org/10.1016/j.jfo.2013.05.008 Google Scholar
- Kulczycki A. [Overcoming Family Planning Challenges in Africa: Towards Meeting Unmet Need and Increasing Service Delivery] . Afr J Reprod Health [Internet]. 2018 Mar [cited 2024 Oct 21];22(1):14-19. French. https://doi.org/10.29063/ajrh2018/v22i1.1 Download ajol-file-journals_49_articles_169831_submission_proof_169831-577-436618-1-10-20180418.pdf. Google Scholar
- Bongaarts J, Hardee K. The role of public sector family planning programmes in meeting contraceptive demand in sub-Saharan Africa . International Perspectives on Sexual and Reproductive Health [Internet]. 2017 June [cited 2024 Oct 21];43(2):41-50. English, French. https://doi.org/10.1363/43e3917 Download pdf to view full text. Google Scholar
- Obuchowski NA. Receiver operating characteristic curves and their use in radiology . Radiology [Internet]. 2003 Oct 1[cited 2024 Oct 27];229(1):3-8. https://doi.org/10.1148/radiol.2291010898 Download pdf to view full text. Google Scholar
- Ahmed S, Choi Y, Rimon JG, Alzouma S, Gichangi P, Guiella G, Kayembe P, Kibira SP, Makumbi F, OlaOlorun F, Omoluabi E, Otupiri E, Oumarou S, Seme A, Shiferaw S, Anglewicz P, Radloff S, Tsui A. Trends in contraceptive prevalence rates in sub-Saharan Africa since the 2012 London Summit on Family Planning: results from repeated cross-sectional surveys . Lancet Glob Health [Internet]. 2019 May 17 [cited 2024 Oct 21];7(7):e904-11. https://doi.org/10.1016/s2214-109x(19)30200-1 Google Scholar
- Damtew SA, Fantaye FT. Women alone modern contraceptive use decision making and its correlates, evidence from PMA CS 2021 survey . BMC Womens Health [Internet]. 2024 Mar 30 [cited 2024 Oct 21];24(1):205. https://doi.org/10.1186/s12905-024-03050-x PubMed | Google Scholar
- Chukwudeh SO, Oduaran A.“My Mother Persuaded Me to Have More Children”, Understanding the Influence of Social Network on Fertility Behavior in Sub-Saharan Africa . Int J Environ Res Public Health [Internet]. 2024 Mar 24[cited 2024 Oct 21];21(4):396. https://doi.org/10.3390/ijerph21040396 PubMed | Google Scholar
- Bearak JM, Popinchalk A, Beavin C, Ganatra B, Moller AB, Tunçalp Ö, Alkema L. Country-specific estimates of unintended pregnancy and abortion incidence: a global comparative analysis of levels in 2015-2019 . BMJ Glob Health [Internet]. 2022 Mar 24 [cited 2024 Oct 21];7(3):e007151. https://doi.org/10.1136/bmjgh-2021-007151 PubMed | Google Scholar
- Ahinkorah BO, Seidu AA, Budu E, Agbaglo E, Adu C, Dickson KS, Ameyaw EK, Hagan JE, Schack T. Which factors predict fertility intentions of married men and women? Results from the 2012 Niger Demographic and Health Survey. PLoS ONE [Internet]. 2021 Jun 9 [cited 2024 Oct 21];16(6):e0252281. https://doi.org/10.1371/journal.pone.0252281 PubMed | Google Scholar
- Fatusi AO, Adedini SA, Mobolaji JW. Trends and correlates of girl-child marriage in 11 West African countries: evidence from recent Demographic and Health Surveys [version 2; peer review: 2 approved] . AAS Open Res [Internet]. [First Version Published: 2021 Jun 22; Latest Version Published: 2021 Sep 1] [cited 2024 Oct 21];4:35. https://doi.org/10.12688/aasopenres.13248.2 PubMed | Google Scholar
- Dhakal S, Song JS, Shin DE, Lee TH, So AY, Nam EW. Unintended pregnancy and its correlates among currently pregnant women in the Kwango District, Democratic Republic of the Congo. Reprod Health [Internet]. 2016 Jun 16 [cited 2024 Oct 21];13(1):74. https://doi.org/10.1186/s12978-016-0195-z PubMed | Google Scholar
- Poudel S, Upadhaya N, Khatri RB, Ghimire PR.Trends and factors associated with pregnancies among adolescent women in Nepal: Pooled analysis of Nepal Demographic and Health Surveys (2006, 2011 and 2016) . PLOS ONE [Internet]. 2018 Aug 9 [cited 2024 Oct 21];13(8):e0202107. https://doi.org/10.1371/journal.pone.0202107 PubMed | Google Scholar
- Mohamed EAEB, Hamed AF, Yousef FMA, Ahmed EA.Prevalence, determinants, and outcomes of unintended pregnancy in Sohag district, Egypt . J Egypt Public Health Assoc [Internet. 2019 Mar 13 [cited 2024 Oct 21];94(1):14. https://doi.org/10.1186/s42506-019-0014-9 PubMed | Google Scholar
- Wado YD, Sully EA, Mumah JN. Pregnancy and early motherhood among adolescents in five East African countries: a multi-level analysis of risk and protective factors . BMC Pregnancy Childbirth [ Internet]. 2019 Feb 6 [cited 2024 Oct 21];19(1):59. https://doi.org/10.1186/s12884-019-2204-z PubMed | Google Scholar
- Dixit P, Ram F, Dwivedi LK.Determinants of unwanted pregnancies in India using matched case-control designs . BMC Pregnancy Childbirth [Internet]. 2012 Aug 11 [ cited 2024 Oct 21];12(1):84. https://doi.org/10.1186/1471-2393-12-84 PubMed | Google Scholar
- Yenealem F, Niberet G. Prevalence and associated factors of unintended pregnancy among pregnant woman in Gondar town, North west Ethiopia, 2014 . BMC Res Notes [Internet]. 2019 Mar 22 [cited 2024 Oct 21];12(1):161. https://doi.org/10.1186/s13104-019-4203-6 PubMed | Google Scholar
- Médecins du Monde. Les déterminants socioculturels et communautaires des grossesses non désirées et des avortements : district de Djibo (Burkina Faso)[ Socio-cultural and community determinants of unwanted pregnancies and abortions : Djibo District Burkina Faso] [Internet]. Paris (France) : Médecins du Monde; 2015 [cited 2024 Ocy 21]. 65 p. French. Download Determinants-GND-Burkina_MdM.pdf.
- Christofides NJ, Jewkes RK, Dunkle KL, McCarty F, Shai NJ, Nduna M, Sterk C. Risk factors for unplanned and unwanted teenage pregnancies occurring over two years of follow-up among a cohort of young South African women . Glob Health Action [Internet]. 2014 Aug 21 [2024 Oct 21]; 7(1):23719. https://doi.org/10.3402/gha.v7.23719 PubMed | Google Scholar
- Gunawardena N, Fantaye AW, Yaya S.Predictors of pregnancy among young people in sub-Saharan Africa: a systematic review and narrative synthesis . BMJ Glob Health [Internet]. 2019 Jun 5 [cited 2024 Oct 25];4(3):e001499. https://doi.org/10.1136/bmjgh-2019-001499 PubMed | Google Scholar