Descriptive analysis of COVID-19 deaths in Kadoma City, Zimbabwe, September 2020 - August 2021
Derek Masokovere1, Daniel Chirundu2, Tsitsi Patience Juru1, Gerald Shambira1, Notion Tafara Gombe1, Mufuta Tshimanga1
1Department of Primary Health Care Sciences: Family Medicine, Global and Public Health Unit, University of Zimbabwe, Harare, Zimbabwe, 2Kadoma City Health Department, Kadoma, Zimbabwe
&Corresponding author
Derek Masokovere, Department of Primary Health Care Sciences, Family Medicine, Global and Public Health Unit, University of Zimbabwe, Harare, Zimbabwe
Introduction:
Globally COVID-19 case fatality rate is estimated to be 2.5%. Zimbabwe recorded the highest case fatality rate (CFR) at 3.5%. No analysis of COVID-19 deaths was done in Kadoma City despite a case fatality rate of 10%. We conducted a descriptive analysis of COVID-19 deaths in Kadoma City from September 2020 to August 2021.
Methods:
A descriptive cross-sectional study was carried out to describe the deaths by person, place and time, clinical characteristics and trends in Kadoma City. Records of COVID-19 deaths were our objects of study. All 129 records were included in the study. The COVID-19 deaths list for Kadoma City was the data source. Variables analyzed include age, sex, signs and symptoms, preexisting conditions and survival time from date of onset. Demographics and clinical characteristics were summarized to come up with medians, frequencies and proportions.
Results:
The median days to death was 3 with interquartile range (IQR) (2-5) and the median age was (IQR) 67 (47-80) years. A total of 97 (75%) deaths occurred in the community and 32 (25%) occurred in isolation centres. The major cause of death was acute respiratory distress syndrome (ARDS) 127 (98%). Majority of the deaths 28 (45%) had diabetes and 28 (45%) had hypertension. The informal employment sector recorded the most deaths 45 (39%). Males were 79 (61%) and females were 50 (39%).
Conclusion:
We concluded that COVID-19 deaths were high among patients isolating at home. ARDS was the major cause of death. The burden was made worse by the cases that were brought in dead. We strengthened surveillance and risk communication.
Introduction

COVID-19 is caused by severe acute respiratory coronavirus 2 (SARS-CoV-2). A COVID-19 death is defined as death resulting from clinically compatible illness in a probable or confirmed COVID-19 case unless there is a clear alternative cause of death that cannot be related to COVID-19 disease [1]. As of 05 November 2021, globally, 504, 753, 890 COVID-19 cases and 5, 260, 476 deaths had been recorded. The first fatalities of the disease were recorded in China then Italy, Spain and the United States of America. To date, all regions of the world have recorded COVID-19 deaths. Globally the case fatality rate of COVID-19 is estimated to be 2.5%. COVID-19 is the 12th leading cause of death in adults in the world. As of 05 November 2021, Africa had recorded an estimated 7.8 million cases and 224,093 deaths, while Zimbabwe had recorded 266, 355 COVID-19 cases and 4, 708 deaths [2]. Death occurs mostly in the elderly, immunocompromised individuals and those with co-morbidities such as diabetes and hypertension [3].
In Zimbabwe, from June to September 2021, an increase in the number of COVID-19 cases was experienced in comparison with the first and second wave [
4]. The increase in cases was associated with a corresponding high case fatality rate (CFR) of 3.5% in the third wave compared to 2.1% in the second wave [
5]. WHO requires that all member states report and register all COVID-19 deaths within 24 hours [
6]. Kadoma City recorded 1 213, COVID-19 cases and 129 deaths between September 2020 and August 2021, which was the highest, compared with the other towns in Mashonaland West Province during the same period. The first case of COVID-19 in Kadoma City was reported on 30 April 2020 and the first death was recorded on 1 September 2020. During the third epidemic wave of COVID-19 infection, the case fatality rate for Kadoma City was 10% which was very high compared with the provincial 2.3% and the National 3.5%. The city strengthened case management, surveillance systems and enforcement of COVID-19 prevention and control measures in a bid to reduce the deaths but the problem persisted. An in-depth analysis of COVID-19 deaths in Kadoma City has not been done. We therefore conducted a descriptive analysis of COVID-19 deaths in Kadoma City from September 2020 to August 2021.
Methods

Study design
A descriptive cross-sectional study using secondary data was carried out to describe the deaths by person, place and time and to describe the clinical characteristics and trends of COVID-19 deaths in Kadoma City.
Study setting
The study was conducted in Kadoma City 140 km south of Harare City in Sanyati District, Mashonaland West Province. According to ZimStat 2021 population projections, Kadoma City has a total population of 114,471 [
1]. The population of Kadoma City constitutes 9% of the provincial population. The city is densely populated with 70% residing in high-density suburbs. Rimuka´s high-density suburb alone is home to 50% of the population. Densely populated areas like Kadoma City are known to promote transmission of COVID-19. There are two hospitals dedicated to the isolation of COVID-19 patients, Kadoma General Hospital offering comprehensive care including COVID-19 isolation and Queen Marry Hospital offering COVID-19 isolation only. Severe cases were isolated in these two hospitals while moderate to mild cases isolated at home according to Ministry of Health and Child Care (MOHCC) COVID-19 case management guidelines. Both isolation centres were managed by Kadoma General Hospital under the administration of MOHCC. Reported COVID-19 deaths were from these two isolation centres and the community.
Study population
Records of COVID-19 deaths from Kadoma city for the period from September 2020 to August 2021 were the study objects. All the 129 death records were included in the study.
Data collection and data source
In Zimbabwe a confirmed COVID-19 case is any person with laboratory confirmation of COVID-19 infection, irrespective of signs and symptoms. A COVID-19 death is defined as death resulting from clinically compatible illness in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19 disease. The COVID-19 deaths line list for Kadoma City for September 2020-August 2021 was used as the data source. The COVID-19 deaths list is kept as an Excel based dataset by the health information office with an objective of estimating the case fatality rate of COVID-19 in Kadoma City. Variables analyzed include age, sex, signs and symptoms, co-morbidities, treatment given, date of diagnosis, date of death and survival time from date of diagnosis (
Figure 1).
Data analysis
Data was analyzed into frequencies, proportions and medians. Trends in COVID-19 deaths were determined and relationship between COVID-19 death and epidemic waves of infection were established. The trends of progression of deaths over time during the study period were analysed. Demographics were summarized to come up with frequencies and proportions. Median age in years were calculated as well as median time to death from day of diagnosis. A spot map showing the patients who died of COVID-19 by place of residence was plotted to show residential areas that were highly affected by COVID-19 deaths.
Ethical Considerations
The study was reviewed and approved by the Mashonaland West Provincial Ethics Committee (JFREC-KC/3/23). Confidentiality of patients´ data was maintained. Deaths records of COVID-19 patients were not shared with third parties
Results
The dataset that was analysed comprised 129 records. Completeness of variables that include age, sex, place of death and date of death was 100%. However, history of travel was 41% (53/129), pre-existing conditions was 48% (62/129), case classification was 96% (124/129) and date of diagnosis was 98% (126/129), complete. All the 129 records (100%) were analysed.
COVID-19 deaths in Kadoma City from September 2020 to August 2021 comprised 79 (61%) males and 50 (39%) females. A total of 97 (75%) deaths occurred in the community and 32 (25%) occurred in isolation centres. All the deaths 129 (100) were residents of Kadoma City with no history of travel in the past 14 days. The median days to death from date of diagnosis was (IQR) 3(2-5) and the median age was (IQR) 67(47-80) years. Most of the deaths were recorded among person working in the informal employment 65 (45%) followed by the unemployed 45 (39%) (
Table 1).
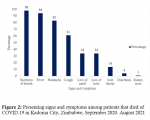
The top three signs and symptoms observed among COVID-19 deaths were shortness of breath, fever and headache. Shortness of breath was present in 126 (98%) of the participants. Fever was reported in 121 (94%) of all the deaths. A total of 101 (78%) of the deaths had headaches (
Figure 2).
Majority of the deaths 28 (45%) had diabetes and 28 (45%) had hypertension. Asthma was recorded in two cases (3%). Those with HIV were two (three percent), tuberculosis and cardiovascular disease were recorded in one death each (
Table 2). The major cause of death was acute respiratory distress syndrome (ARDS) 127 (98%). There was no data on the cause of death for two (two per cent) of the deaths.
Paracetamol, ceftriaxone and zinc sulphate were administered to cases in both home/community isolation and institutional isolation. However, those in institutional isolation were additionally given oxygen supplementation. Paracetamol, Ceftriaxone, Vitamin C and dexamethasone were administered to 90 (70%) of individuals on the death list. Oxygen supplementation was administered to 32 (25%) of all the death cases. All cases that were administered oxygen supplementation were in institutional isolation. A total of 39 (30%) deaths happened at home without prior diagnosis for COVID-19. These were brought in dead (BID) at the hospital mortuary. These BIDs were only confirmed as COVID-19 cases after death.
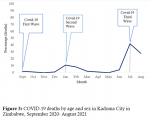
In 2020, COVID-19 deaths were kept below four percent from September to December. The highest number of deaths 54 (42%) were recorded in July 2021. In August 2021 38 (30%) of the deaths were recorded. January and February 2021 recorded 14 (11%) and 10 (8%) deaths respectively. (
Figure 3)
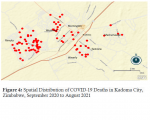
Rimuka high density suburb recorded the most deaths contributing 62 (48%) of all the COVID-19 deaths in Kadoma City. Waverly, Ingezi and Chemukute high density suburbs recorded 9 (7%) of the deaths each respectively. The remaining residential areas recorded less than 5% of all the COVID-19 deaths each. The spatial distribution of COVID-19 deaths in Kadoma City is presented in
Figure 4.
Discussion
We analysed demographic and clinical characteristics of COVID-19 deaths in Kadoma City, Zimbabwe. The main findings were that most of the dead COVID-19 cases were the elderly, occurred in the community and acute respiratory distress syndrome (ARDS) was the major cause of death. The median age at death was 67 years but majority were within the over 64 years age group, therefore there is a need for extra care and protection of this age group to reduce mortality. Furthermore, the greater than 65 years age group is related to developing and dying of viral infectious diseases like COVID-19. The findings were similar with Van Wyk et. al. (2020). Most of the elderly also had chronic conditions, which in turn worsened COVID-19 and increased their risk of dying. This was consistent with findings reported by Van Wyk et. al. (2020) [7].
The burden of death was high in the community/home isolation compared with those in hospital isolation. COVID-19 patients in hospital isolation were subjected to continuous monitoring and care and were administered with oxygen supplementation when facing difficulty in breathing whereas monitoring of patients in the community were disrupted by lack of resources such as transport and was sometimes done over the phone without physical assessment of the patients. The findings were similar with Jaasat et. al. (2021)[
8].
Acute respiratory distress syndrome (ADRS) was a major cause of death in COVID-19 patients. Shortness of breath, fever and headache were the three most common signs and symptoms in patients who died of COVID-19. Fever and respiratory disorders are the two cardinal signs that have been reported in almost every region of the world in patients suffering from COVID-19. It is key to continuously monitor the progression of fever and shortness of breath in COVID-19 patients. The findings were consistent with Qui et. al. (2021)[
9].
COVID-19 fatalities were high in individuals who were tested in post-mortem compared to cases that were being followed as part of active monitoring initiatives and surveillance. The proportion of brought-in dead (BID) confirmed after death may represent the proportion of missed cases in the community. Surveillance teams were overwhelmed due to the growing number of new cases and limited resources. The teams faced challenges in follow-up cases and contacts as well as testing of all exposed individuals. This was consistent with findings by Skrip et. al. (2020)[
10].
The case fatality rate was high in males compared to females both in isolation and in the community. Chances of exposure to COVID-19 in males were increased by their occupation and economic activities. Most of the man are employed in the informal sector and could not stay at home during lockdowns. This could have resulted in increased chances of exposure and dying of COVID-19. The findings were similar with Jaasat et. al. (2021) [
8]. Majority of the dead worked in the informal sector compared to other professions. Individuals in the informal sector often work in overcrowded facilities such as markets and small-scale mines where adherence to infection prevention and control (IPC), physical distancing, hand sanitising and the wearing of masks were minimum and sometimes difficult.
Most deaths occurred within the first week from date of diagnosis. This could have been a result of late health seeking behaviour. There was fear of stigma and discrimination after contracting COVID-19 therefore suspected cases would take some time to present themselves for diagnosis and would sometimes present when the condition has already complicated. This was similar to findings by Nachega et. al. (2020)[
11].
Hypertension and diabetes were the two leading co-morbidities reported in patients who died of COVID-19. The conditions were also common in the elderly who were constituted most of the deaths. Hypertension and diabetes were recorded as important co-morbidities related to COVID-19 deaths in all regions of the world. The findings were consistent with Mwananyanda et. al. (2021)[
12]. Treatment of majority of patients who died of COVID-19 was according to the national COVID-19 case management guidelines using a combination of paracetamol, Ceftriaxone, Vitamin C, Dexamethasone and Zinc sulphate.
Most COVID-19 deaths occurred during the third and second epidemic waves of infection. The second wave of COVID-19 infections was because of complacency in prevention and control measures during the festive season. This saw a lot of people being infected and dying of COVID-19 in the weeks preceding the festive period. The third wave of infection was also a result of complacency in prevention and control measures and the circulation of the fast-spreading and lethal Delta variant. The findings were also similar to Van Wyk et. al. (2020) [
7]. The majority of the deaths were recorded in Rimuka high-density suburb. Almost half of Kadoma City´s population are residents of Rimuka high-density suburb. The population density in this residential suburb could have facilitated the spread and death of COVID-19.
The data set had missing data on comorbidities for some deaths thereby affecting data analysis, completeness of data and reporting. Date of onset of signs and symptoms was not captured in the dataset. Therefore, the date of diagnosis was assumed to be the date of onset.
Conclusion
We concluded that the COVID-19 deaths were high in the elderly above the age of 64 in both males and females. Death was high in the community compared to hospitalised patients and acute respiratory distress syndrome (ARDS) was the major cause of death. Furthermore, the burden of death was made worse by BIDs that were not picked up during surveillance. We recommended mobilisation of resources and strengthening of surveillance teams to enable daily monitoring of all patients and active case finding. There is need to strengthen case management for the elderly above the age of 64 years, patients with fever, shortness of breath, diabetes and hypertension. However, despite having close to half of the population further studies are required to determine factors associated with COVID-19 death in Rimuka high density suburb.
What is known about this topic
- COVID-19 is caused by coronavirus SARS-CoV-2
- Signs and symptoms include fever, cough, sore throat, headache, loss of taste or smell
- Complications include respiratory failure and multi organ failure
What this study adds
- The study established groups of individuals who are at risk of severe illness in Kadoma City and come up with ways of protecting them
- Furthermore, the study established deaths were higher in in-home than in institutional isolation. This finding makes routine follow up of patients in-home isolation imperative to monitor severity of disease thereby reducing deaths
Competing interests
The authors declare that they have no competing interests.
Permission to publish
Permission to publish the article was obtained.
Funding declaration
Funding for this article was from personal sources.
Ethical consideration
The study was reviewed and approved by the Mashonaland West Provincial Ethics Committee (JFREC-KC/3/23). Permission to carry out the study was obtained from Kadoma City Health Directorate and the Medical Superintendent for Kadoma general hospital. Names of the study participants were not included on the data extraction form. The data extraction forms and the deaths list were kept under lock and key. Data from the study participants were not shared with third parties
Authors' contributions
DM, DC, TPJ, GS, NTG, MT participated in conceiving the concept for this study. DC, TJ, GS, AC, NTG and MC supervised the study. DM wrote the first draft of the manuscript. DM, DC, TPJ, GS, NTG, MT revised, edited and approved the final version of the manuscript.
Acknowledgments
We acknowledge the Medical Superintendent and Matron Kadoma General Hospital, Health Information Officer Sanyati District and Health Information Clerk Kadoma City Health. Special thank you to Addmore Chadambuka for his mentorship and expert review of various drafts of this manuscript.
Tables and figures
Table 1: Demographic characteristics of COVID-19 deaths, Kadoma City, September 2020 - August 2021
Table 2: Comorbidities and treatment received by patients who died of COVID-19, Kadoma City, September 2020-August 2021 (n=129)
Figure 1: Flow diagram for isolation of COVID-19 patients
Figure 2: Presenting signs and symptoms among patients that died of COVID-19 in Kadoma City, Zimbabwe, September 2020- August 2021
Figure 3: COVID-19 deaths by age and sex in Kadoma City in Zimbabwe, September 2020- August 2021
Figure 4: Spatial Distribution of COVID-19 Deaths in Kadoma City, Zimbabwe, September 2020 to August 2021
References
- Kadoma City Health Department. Kadoma City COVID-19 Situational report. Kadoma (Zimbabwe):Kadoma City Health Department; 2021. Google Scholar
-
Worldometer: COVID-19 Coronavirus Pandemic [Internet]. [place unknown]: Worldometers.info; [cited 2021 Nov 5]. PubMed | Google Scholar
- Guilmoto CZ. COVID-19 death rates by age and sex and the resulting mortality vulnerability of countries and regions in the world . MedRxiv [Preprint]. medRxiv 2020.05.17.20097410 2020 [posted 2020 May 20; cited 2024 Sep 2]. https://doi.org/10.1101/2020.05.17.20097410 PubMed | Google Scholar
- Murewanhema G, Burukai T, Mazingi D, Maunganidze F, Mufunda J, Munodawafa D, Pote W.A descriptive study of the trends of COVID-19 in Zimbabwe from March-June 2020: policy and strategy implications . Pan Afr Med J [Internet]. 2020 Nov 9 [cited 2024 Sep 2];37(Suppl 1):33. https://doi.org/10.11604/pamj.supp.2020.37.1.25835 PubMed | Google Scholar
- Matthew M, Chingono F, Mangezi S, Mare A, Mbazangi S.Hidden variables to COVID 19: Zimbabwe. Version 1. Cambridge Open Engage [Preprint]. [posted 2020 Sep 14; cited 2024 Sep 2]. https://doi.org/10.33774/coe-2020-1mqnz PubMed | Google Scholar
- Hu Y, Deng H, Huang L, Xia L, Zhou X. Analysis of characteristics in death patients with covid-19 pneumonia without underlying diseases . Academic Radiology [Internet]. 2020 Apr 7 [cited 2024 Sep 2];27(5):752. https://doi.org/10.1016/j.acra.2020.03.023 PubMed | Google Scholar
- Wyk VP van, Bradshaw D, Groenewald P, Seocharan I, Manda S, Roomaney RA, Awotiwon O, Nkwenika T, Gray G, Buthelezi SS, Mkhize ZL.COVID deaths in South Africa: 99 days since South Africa´s first death . South African Medical Journal [Internet]. 2020 Oct 1 [cited 2024 Sep 2];110(11):1093-9. http://dx.doi.org/10.7196/samj.2020.v110i11.15249 PubMed | Google Scholar
- Jassat W, Brey Z, Parker S, Wadee M, Wadee S, Madhi SA.A call to action: Temporal trends of COVID-19 deaths in the South African Muslim community . South African Medical Journal [Internet]. 2021 Jun 15 [cited 2024 Sep 2];111(8):692-4. http://dx.doi.org/10.7196/samj.2021.v111i8.15878 PubMed | Google Scholar
- Qiu P, Zhou Y, Wang F, Wang H, Zhang M, Pan X, Zhao Q, Liu J. Clinical characteristics, laboratory outcome characteristics, comorbidities, and complications of related COVID-19 deceased: a systematic review and meta-analysis . Aging Clin Exp Res [Internet]. 2020 Jul 30 [cited 2024 Sep 2];32(9):1869-78. https://doi.org/10.1007/s40520-020-01664-3 PubMed | Google Scholar
- Skrip L, Derra K, Kaboré M, Noori N, Gansané A, Valéa I, Tinto H, Brice BW, Gordon MV, Hagedorn B, Hien H, Althouse BM, Wenger EA, Ouédraogo AL. Clinical management and mortality among COVID-19 cases in sub-Saharan Africa: A retrospective study from Burkina Faso and simulated case analysis . International Journal of Infectious Diseases [Internet]. 2020 Sep 25 [cited 2024 Sep 2];101:194-200. https://doi.org/10.1016/j.ijid.2020.09.1432 PubMed | Google Scholar
- Nachega JB, Ishoso DK, Otokoye JO, Hermans MP, Machekano RN, Sam-Agudu NA, Bongo-Pasi Nswe C, Mbala-Kingebeni P, Madinga JN, Mukendi S, Kolié MC, Nkwembe EN, Mbuyi GM, Nsio JM, Mukeba Tshialala D, Tshiasuma Pipo M, Ahuka-Mundeke S, Muyembe-Tamfum JJ, Mofenson L, Smith G, Mills EJ, Mellors JW, Zumla A, Mavungu Landu DJ, Kayembe JM.Clinical characteristics and outcomes of patients hospitalized for COVID-19 in Africa: early insights from the Democratic Republic of the Congo . The American Journal of Tropical Medicine and Hygiene [Internet]. 2020 Oct 2 [cited 2024 Sep 2];103(6):2419-28. https://doi.org/10.4269/ajtmh.20-1240 PubMed | Google Scholar
- Mwananyanda L, Gill CJ, MacLeod W, Kwenda G, Pieciak R, Mupila Z, Lapidot R, Mupeta F, Forman L, Ziko L, Etter L, Thea D.Covid-19 deaths in Africa: prospective systematic postmortem surveillance study . BMJ [Internet]. 2021 Feb 17 [cited 2024 Sep 2];372:n334. https://doi.org/10.1136/bmj.n334 PubMed | Google Scholar