Measles Outbreak in Lambu Internally Displaced Persons´ Camp, Maiduguri, Borno State, Nigeria, 2017
Taiwo Israel Olasoju1,2, Mary Idowu Olasoju3, Batula Bishara Daggash1,4, Bio Belu Abaye1,5, Chibuike Enumah1, Salisu Isah1,6, Mohammed Tahiru Bolori7, Oluwawemimo Oluseun Adebowale3
1Nigeria Field Epidemiology and Laboratory Training Program (NFELTP), 2Department of Veterinary and Pest Control Services, Federal Ministry of Agriculture and Rural Development, Area 11, Garki, Abuja, FCT, Nigeria, 3Department of Veterinary Public Health and Preventive Medicine, College of Veterinary Medicine, Federal University of Agriculture, Abeokuta, Ogun State, Nigeria, 4Department of Medical Microbiology, University of Maiduguri Teaching Hospital, Maiduguri, Borno State, Nigeria, 5Epidemiology Division, Public Health Department, Bayelsa State Ministry of Health, Ba yelsa State, Nigeria, 6Bauchi State Primary Health Care Development Agency, Bauchi, Bauchi State, Nigeria, 7Department of Community Medicine, University of Maiduguri, Maiduguri, Borno State, Nigeria
&Corresponding author
Mary Idowu Olasoju, Department of Veterinary Public Health and Preventive Medicine, College of Veterinary Medicine, Federal University of Agriculture, Abeokuta, Ogun State, Nigeria.
Introduction:
Measles, a highly infectious disease caused by the Measles virus, is endemic in Nigeria. Although children are vaccinated against measles at the age of nine months which has led to a significant reduction in morbidity and mortality, Nigeria still ranks among the top countries with endemic and uninterrupted transmission of measles infection yearly in Sub-Saharan Africa. This study was carried out to confirm the existence of a measles outbreak, characterize the outbreak in place, person, and time and identify factors associated with the outbreak in Lambu Internally-Displaced Persons' (IDP) camp, Maiduguri, Nigeria.
Methods:
An unmatched case-control study was conducted among children living in Lambu internally displaced persons (IDP) camp. A suspected case was any person with fever and generalized maculopapular rash and cough, coryza, or conjunctivitis in Lambu IDP camp between February 13 to March 7, 2017. A pre-tested interviewer-administered structured questionnaire was used to gather information on demographic characteristics, socio-economic status, educational status, and potential associated factors. Specimens from five cases were collected and sent to a laboratory for confirmatory diagnosis. An active case search in health facilities close to the Camp was performed. The epidemic curve was drawn, and the odds ratio was calculated at a 95% confidence interval using Epi Info version 7.2
Results:
The first case was a 12-month-old girl who presented with fever, nasal discharge, conjunctivitis and generalized rashes. A total of 28 cases were identified. The outbreak lasted for 3 weeks between February 13, 2017, and March 7, 2017, with 3 deaths. The median age of cases was 48 (IQR: 24-60) months. Eighteen cases (18/28=64.3%) were 12-59 months old, while six (6/28=21%) were aged 5 to 9 years. Two of the 3 (66.7%) deaths were reported in under-five children. Three out of the five samples collected for laboratory analysis were positive for Measles virus. Measles vaccination coverage was low. Only 3 of the 28 cases (10.7%) and 4 of the 48 controls (8.5%) had received measles vaccine before the outbreak. Eligible children were offered reactive measles vaccination during the outbreak. Residing close (<5km) to a health facility was associated with lower odds (aOR=0.083, 95%CI: 0.008-0.460) of developing measles and so was a prior visit to a health facility for a previous illness episode (aOR=0.127, 95%CI: 0.003-0.976).
Conclusion:
There was an outbreak of measles among children in Lambu IDP camp and the instituted control measures included reactive vaccination. The infection was introduced to the IDP camp by children with low or zero immunization coverage from hard-to-reach settlements. Community sensitization on measles and immunization was done.
Introduction

Globally, measles infects 20 million people and is responsible for over 410,000 mortalities annually, though mainly among children less than 5 years. This is indeed a great achievement for a disease that was earlier responsible for over two million global annual deaths. The introduction of measles vaccination, one of the most cost-effective health interventions ever produced has caused a significant reduction of this [1,2]. About 17.1 million deaths were prevented by measles vaccinations administered between 2000 and 2014 [3]. However, measles continues to cause high morbidity and mortality among children worldwide, despite the availability of a safe, effective, and low-cost vaccine. It costs less than one US dollar to vaccinate a child against measles. The disease has been referred to as the most recurrent cause of vaccine-preventable childhood death, worldwide [4, 5].
Measles is a human disease and is not known to occur in animals nor is there any known environmental reservoir of the infection. The disease is characterized by a prodrome of fever (as high as 40.5°C/105°F), malaise, cough, coryza, and conjunctivitis (the three “Cs”), pathognomonic enanthema (Koplik spots) followed by a maculopapular rash. The rash usually appears about 14 days after a person is exposed; however, the incubation period ranges from 7 to 21 days. The rash spreads from the head to the trunk and then, to the lower extremities. Patients are considered to be contagious from 4 days before to 4 days after the rash appears [
6].
Borno State in northeast Nigeria has experienced repeated measles outbreaks. From February to May 2023, more than 50 children died as a result of measles epidemics caused by an inflow of unvaccinated children from difficult-to-reach and extremely difficult-to-reach communities in northeast Nigeria. Borno State was the most affected, with over 5,000 suspected cases by the end of May 2023, with Jere LGA and Maiduguri Metropolitan Council having 1,644 and 1,627 cases, respectively. Yobe State had 917 suspected cases of measles, with 9 fatalities from measles-related complications, while Adamawa State had 66 suspected cases of measles. [
7].
Risk factors for contracting measles include not being vaccinated against the disease, overcrowding in a household, lack of compliance with routine immunization schedule, and acquired or inherited immunodeficiency state [
8,
9]. The case fatality rates (CFR) of measles in Africa generally range from 3% to 5% but can be as high as 30% during severe outbreaks [
10].
We report on a 2017 measles outbreak investigation in Lambu internally displaced persons (IDP) camp. On 3 March 2017, the disease response team received an alert from the Borno State Epidemiologist, about an outbreak of Measles in Lambu IDP camp in Jere LGA of Borno State. Subsequently, the team visited the Local Government Area (LGA) headquarters to mobilize the LGA team and also visited the affected camp. We investigated to confirm this outbreak, characterize it in person, place and time, identify associated factors for this outbreak and provide technical support to control the outbreak.
Methods

Study area
Borno State is situated in Northeastern Nigeria. It has 27 Local Government areas (LGA). It is bordered by 3 countries (Chad, Cameroon and Niger) and 3 Nigerian States (Yobe, Adamawa and Gombe states). Jere local government area is one of the two local government areas that form Maiduguri town. Lambu IDP camp was a new unofficial camp set up two months before the outbreak in the old Maiduguri area of Jere LGA. The IDP housed people mainly from Mafa and Marte.
The camp had about 800 people who were peasants and largely indigent families from extremely rural areas who were displaced following the insurgency that affected their communities (
Figure 1). The majority were women and children, many of whom had features of malnutrition. The camp was made up of make-shift overcrowded shelters, most having a single opening as a door. Shallow pits dug by the camp dwellers were the initial latrines. The water supply was from an open well also dug by the camp dwellers with multiple containers used to draw water. By the time of this investigation, corporate bodies such as the Norwegian Refugee Council had started providing boreholes, and better temporary shelters, safer water supply and housing respectively.
Study Design
An unmatched case-control study.
Study population
The study population was defined as children aged 6 months to 15 years living in Lambu IDP camp.
Case Definition
A suspected case was any person with fever and generalized maculo-papular (non-vesicular) rash and cough, coryza or conjunctivitis (red eyes) or any individual in whom a clinician suspects measles in Lambu IDP camp between February 13 to March 7, 2017 [
11].
On the other hand, a confirmed case was a suspected case with laboratory confirmation (positive IgM antibody) or epidemiological linkage to a confirmed case in an outbreak in Lambu IDP camp between February 13 to March 7, 2017.
We defined a control as any child without measles living in Lambu IDP camp between February 13 to March 7, 2017.
Active Case Search
Active case search was done in the entire Lambu IDP camp using the case definition above. A similar search was done in Dalaram Primary Health Care (PHC), the closest healthcare facility to Lambu camp. The PHC registers were checked for patients who had a rash as possible suspected measles cases managed there. This facility search was done retrospectively for one month.
For each case, data on the age, sex, residence, socio-economic status and time of onset were gathered using a structured interviewer-administered questionnaire. The incidence by age and sex was determined and an epidemic curve was drawn.
Sample Size and Sampling Technique
The research utilized all 28 suspected cases identified in the camp, sourced from the Immediate Case-based Surveillance Reporting Form (IDSR 001C). Two neighbourhood controls were randomly selected for every case. A total of 56 controls were approached however only 48 consented and participated in the study.
Data collection
An interviewer-administered structured questionnaire was used to collect information from the participants. The line list form provided twenty-eight cases with the following variables: ID number, Ward, settlement, Name, Sex, Date of birth or age, Date of onset of rash, Number of valid vaccine doses, Blood taken for laboratory analysis, Results of laboratory analysis, Disease outcome and comments.
We generated a hypothesis from the literature that a measles outbreak in Lambu IDP camp could be due to low immunization coverage. To test this hypothesis, we carried out an unmatched case-control study at the IDP camp. The study population was defined as children aged 6 months to 15 years living in Lambu IDP camp and information regarding potential risk factors was gathered through an interviewer-administered questionnaire. Comparison between cases and controls for the different potential associated factors was done using Epi Info version 7.2 and Health Mapper version 4.3. The odds ratio and corresponding 95% confidence intervals were reported.
Laboratory Investigations
Five measles-positive cases were randomly selected and blood specimens were collected from them. The blood samples were sent to the WHO Measles and Yellow Fever Laboratory, Gombe State for testing using an enzyme-linked immunosorbent assay technique to screen for Measles IgM.
Ethical considerations
Since this was an outbreak situation, the Director, Public Health Department, State Epidemiologist and other officers in the State Ministry of Health approved the outbreak investigation and response. Written informed consent was obtained from all respondents and from their guardians in case of minors.
Results
Descriptive studies
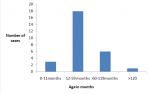
The index case was a 12-month-old girl who the parents revealed had not been vaccinated against measles and had immigrated from Kala town of Mafa LGA with her parents and developed symptoms on, February 13, 2017. At the time of investigation, the symptoms observed in the index case included fever, nasal discharge, conjunctivitis and generalized rashes. A total of 28 cases were recorded between February 13, and March 8, 2017. The median age was 48 months with an interquartile range (IQR:24-60). A total of 3 deaths were recorded. Eighteen cases (18/28=64.3%) were within 12-59 months of age and six cases (6/28=21.4%) were within 5-9 years (
Figure 2 ) and the ratio of males to females cases was 1:1 (
Table 1). Two (2/3=66.7%) of the deaths were under 5 years of age, specifically among the 12-59 months age group. The other fatal case was within the 5-9 years age group. There were no deaths among children aged 10 years and above (
Table 1). Cases were recorded from 13 February 2017, and the outbreak spanned for about 3 weeks (up to March 8, 2017), with multiple peaks during this period (
Figure 3). Notification for the outbreak was sent on March 2, 2017, to the LGA. The first death case was recorded on March 2, 2017. Lege ward recorded the highest number of cases, 26; while Shamuri and Kaula wards had a single case each.
Epidemiological characteristics and vaccination coverage of the affected population
A total of 76 children participated in this study: 28 (36.8%) cases and 48 (63.2%) controls. The caregivers, mostly mothers were the respondents. Many of the responding parents were married, with 92.9% (26/28) cases and 89.6% (43/48) controls. Most of the children were aged 12-59 months, with 64.3% (18/28) cases compared to 52.1% (25/48) controls. There were 50.0% (14/28) male cases and, 52.1% (25/48) male controls. The majority ethnicity for cases was Kanuri (92.9%, 26/28) and for controls it was Shuwa Arab (64.6%, 31/48). There were only 3 Hausa participants, and all were controls (3/48, 6.3%). Before the outbreak, 3 of the 28 cases (10.7%) had received Measles vaccination compared to 4 of the 48 controls (8.3%) (
Table 2). Despite a response by the Borno State Government, and partners, only 15 of the studied cases and 17 of the controls received reactive vaccinations. Three out of the five samples (60%) collected for laboratory analysis were positive for Measles IgM.
Factors associated with the measles outbreak
There was no significant association between a child who was immunized during the last supplementary immunization activity (SIA) and the development of measles (aOR=1.661, 95% CI: 0.207-11.862). Our study findings also suggest a relationship between the number of children living in a room and having measles infection but it was not statistically significant, (aOR= 0.64, 95%CI: 0.20 - 2.06). Children who resided less than 5km away from the nearest health facility were significantly less likely to develop measles compared to those who resided 5-20km from the nearest health facility, (aOR=0.08, 95% CI: 0.01-0.46). Having a prior illness that resulted in visiting a healthcare facility was significantly protective against measles (aOR=0.127, CI: 0.003 - 0.976, (
Table 3)). Notably, 66.7% (32/48) of control mothers had received Quranic education compared to only 3% among the case mothers.
Discussion
Our investigation established a measles outbreak in the Lambu IDP camp in Jere local government area of Borno State. The inhabitants of the camp migrated from Mafa local government area of the State.
The confirmation of an ongoing acute Measles infection is supported by the fact that 60% of the samples submitted to the laboratory were positive for Measles IgM. The two samples that tested negative could have come from cases whose onset of rashes started earlier than the other positive cases with acute infections, given that all the recruited cases fulfilled the conditions listed in the case definition and previous research also indicates occurrence of symptoms showed a positive association with the serological results [
12].
The epi curve of the outbreak indicates that there was no herd immunity in the community though, the virus appears to have encountered initial hindrances from spread, perhaps before the index case came in contact with another susceptible individual(s). The remaining part of the curve from March 2 exhibits a classic typical measles epi curve, characterized by a rapid increase in the number of cases followed by a gradual decline. The curve indicates a sharp peak as the infection spreads rapidly through the susceptible population corresponding to the measles virus's highly contagious nature. Location of susceptible individuals and contact with infected child in the community per time results in localized outbreaks and subsequent peaks as observed in the latter part of the epi curve. Secondary transmission from initially infected cases could also have been responsible for the additional waves of cases, causing multiple peaks on the epi curve as new chains of transmission were established. The low peaks after the first sharp peak fell within the period of intervention and implementation of control measures such as isolation of cases and contact tracing by the state and outbreak investigation team assisted by other relevant stakeholders present at the IDP camp. This pattern is similar to what was previously reported [
13,
14].
The local health care facility near the IDP camp identified the suspected cases of measles, from where the disease was reported to the state health care authorities after which the state Epidemiologist notified the national healthcare authority on the same day. However, the epi curve reveals that the disease had already been lingering within the community for about two weeks (the index case started showing symptoms on February 13 before it was reported to the LGA health authority (March 2), which triggered the reporting line and action. The peculiarities of the outbreak location, being an IDP camp, and the study population, characterized by over-crowding, low prophylactic vaccination with resultant low immunization coverage, and limited resources, further compounded the situation. These factors contributed to the eventual spread of the disease within the community.
This study, therefore, highlights the presence of a reporting channel, but emphasizes the lack of prompt detection and reporting, as the state authorities did not identify the outbreak until two weeks after it´s incursion into the community as against the WHO recommendation of prompt reporting of measles cases within 24 hours of incursion. [
15]
The majority of the affected children were less than five years of age, while almost all affected children were less than 10 years of age which is consistent with other findings, including a recent report of the outbreak in Sokoto and Bauchi States [
16,
17,
]. A number of other studies agree that the highest prevalence of measles is among the under-five year children, including confirmation of measles children who were less than 9 months [
18,
19].
Findings from the line list form suggested the outbreak in Lambu IDP camp was a result of the children never being vaccinated against Measles. The low vaccine coverage among the participants (9%) might be as a result of a number of factors which may include vaccine hesitancy, lack of access, misinformation, health care system challenges [
20,
21,
22,
23,
24].
The rejection of reactive vaccination by some caretakers/parents of affected children indicates a lack of awareness among respondents. Additionally, the low number of vaccinated children before the outbreak highlights the necessity for more outreach sessions to promote herd immunity among at-risk age groups. Partners may also want to utilize these outreach activities to enhance measles virus surveillance among the population and similar groups.
Both sexes were uniformly affected in the outbreak. The implication of this observation is significant for understanding the epidemiology and transmission dynamics of measles. It indicates that factors such as biological sex or gender do not play a significant role in determining susceptibility to the virus. This is similar to another finding in Sokoto [
16] and it underscores the importance of inclusive and equitable healthcare policies and interventions.
There is a significant burden of measles in Jere LGA, as recently reported by the United Nations Office [
7]. The Lege ward, being a difficult-to-reach area within the LGA, faces typical challenges associated with such terrains, resulting in a negative impact on healthcare provision.. This accounts for the study´s finding showing that the ward recorded the highest number of cases, while Shamuri and Kaula wards had a single case each. Research indicates that low immunization coverage in hard-to-reach communities can lead to outbreaks, as seen in Laos where delays in case notification and low vaccine coverage contributed to a measles outbreak in a hard-to-reach village [
25]. Selective vaccination campaigns has also been suggested for more effective control outbreaks in hard-to reach settings like this [
26].
Our study suggests an association between the number of individuals sharing a room and the likelihood of developing measles during the outbreak, though it was not statistically significant. This finding aligns with earlier research, which consistently demonstrates a positive correlation between overcrowding and measles infection. Specifically, studies have shown that environments with high population density, such as households where multiple individuals share a single room, create optimal conditions for the transmission of measles. This is because measles is highly contagious, spreading through respiratory droplets when an infected person coughs or sneezes. In overcrowded settings, the close and prolonged contact among individuals facilitates the rapid spread of the virus. For example, a systematic review by Baker et al. (2013) highlighted that household crowding significantly increases the risk of measles transmission, particularly in settings where children are in close proximity to one another [
27].
This study identified a statistically significant protective association which proximity to the nearest health facility offers against measles infection. This finding is consistent with other studies, [
8,
9,
28]. Children living farther from health facilities are less likely to receive timely vaccinations, this is because when facilities are distant, caregivers may face challenges in taking their children for regular immunizations. Furthermore, in the event of a measles outbreak, children living far from health facilities may experience delays in receiving medical attention. Prompt treatment can mitigate the severity of the disease and reduce transmission rates. It should also be noted that the further a caregiver lives from a health facility, the greater the logistical challenges, such as transportation costs and time. These barriers can discourage regular health visits, leading to lower immunization rates and higher susceptibility to measles during outbreaks. In its, guidelines for universal health coverage, WHO emphasizes that all individuals and communities should have access to the full range of essential health services without financial hardship and also encourages countries to develop healthcare infrastructure that ensures no one is left more than a one-hour travel distance from a health facility [
29]
Our study revealed that children who experienced a prior illness and visited a healthcare facility were less likely to have measles. These visits provide an opportunity for health workers to improve the knowledge of the caregivers about measles as healthcare providers often use the opportunity to sensitize them on the prevention of various vaccine-preventable diseases. A number of studies demonstrate the importance of healthcare providers sensitizing the caregivers on vaccine preventable diseases when the latter visit the health facility and how recent receipt of immunization messages was found to significantly impact on measles infection [
30,
31].
Our study findings may have been impacted by the following limitation. There was widespread hesitancy among households to disclose cases or participate in this study, which may have affected the number of cases line-listed and their representatives to all measles cases in the study community, though our team consequently made frantic efforts to sensitize the community on the benefits of the study and wider response activities. There was no fixed health post in the camp which made it difficult for us to gather precise information on case management, we instead visited the nearest primary health center as part of the line listing and information-gathering efforts. Number of valid vaccine doses received were not available at time of this publication.
Conclusion
There was an outbreak of measles in Lambu IDP camp predominantly affecting children below 5 years of age. Sharing a room was not a significant contributing factor to the outbreak, while immunization coverage was notably low among participants. Prior contact with a health facility due to a previous illness and living near a health facility were protective factors. This study highlights the need for strengthening disease surveillance, improving community awareness, and ensuring high vaccination coverage in IDP camps and similar settings. By addressing these gaps, healthcare authorities can enhance their ability to promptly detect and respond to outbreaks, ultimately preventing the loss of lives and mitigating the impact of such public health emergencies.
What is already known about this topic
- Measles is a vaccine-preventable disease and therefore its outbreak can be effectively averted with 83% -95% herd immunity
- Measles is highly contagious and the risk of transmission can increase with the number of people sharing a room.
What this study adds
- Situating health facilities within a 5km radius of each community will significantly reduce the incidence of measles even in communities where vaccine hesitancy is prevalent
- Utilizing the presence of caregivers in health facilities to educate them about vaccine-preventable diseases, such as measles can influence the occurrence of these diseases
Competing interests
The authors declare no competing interests.
Authors' contributions
TO conceived and designed the study. TO, BD, BA, CE, SI and MTB conducted the study and performed data collection. TO, MO and BA performed data analysis. TO and MO wrote the manuscript draft. TO. MO. BA and OOA revised the manuscript. All authors have read and approved the final version of the manuscript.
Tables and figures
Table 1: Cases and Deaths by age group and gender in the Measles outbreak in Lambu IDP camp, Jere LGA, Borno State, 2017
Table 2: Socio-demographic characteristics of cases and controls in Lambu IDP camp Borno state, measles outbreak, 2017
Table 3: Factors associated with measles infection among children aged 6 to 180 months in Lambu IDP camp, Borno state, 2017
Figure 1: Map of Borno State showing Measles outbreak location (inset map of Nigeria)
Figure 2: Age distribution of Measles cases in Lambu IDP camp, Jere LGA, Borno State, February-March, 2017
Figure 3: Epi curve of Measles outbreak in Lambu IDP camp, Jere Local Government Area, Borno State, February-March, 2017
References
- Perry RT, Halsey NA. The clinical significance of measles: a review . Orenstein WA, editor. The Journal of Infectious Diseases [Internet]. 2004 May 1 [cited 2024 May 29];189(Supplement_1):S4-16. https://doi.org/10.1086/377712 Google Scholar
- WHO. Measles vaccination has saved an estimated 17.1 million lives since 2000. Geneva (Switzerland): WHO; 2015 Nov 12[cited 2024 Jun 05].
- Caserta MT. Measles (Rubeola; Morbilli; 9-Day Measles).In: Porter RS and Kaplan JL, editors. The Merck Manual Online [Internet]. Whitehouse Station (NJ): Merck Sharp & Dohme Corp; c2010-2011[content last modified 2009 November; cited 2013 September].
- Grais RF, Dubray C, Gerstl S, Guthmann JP, Djibo A, Nargaye KD, Coker J, Alberti KP, Cochet A, Ihekweazu C, Nathan N, Payne L, Porten K, Sauvageot D, Schimmer B, Fermon F, Burny ME, Hersh BS, Guerin PJ.Unacceptably high mortality related to measles epidemics in niger, nigeria, and chad . Cutts FT, editor. PLoS Med [Internet]. 2007 Jan 2 [cited 2024 May 27];4(1):e16. https://doi.org/10.1371/journal.pmed.0040016 PubMed | Google Scholar
- Moss WJ.Measles . Lancet [Internet]. 2017 Jun 30[cited 2024 Jun 6];390(10111):2490-2502. https://doi.org/10.1016/S0140-6736(17)31463-0 Subscription or purchase required to view full article. Google Scholar
- Gastanaduy P, Haber P, Rota Paul A, Manisha P. Measles. In: Hall E, Wodi PA, Hamborsky J, Morelli V, Schillie S, editors. Epidemiology and Prevention of Vaccine-Preventable Diseases [Internet]. 14th ed. Washington (DC): Public Health Foundation; 2021[last reviewed 2021 Aug 18; cited 2024 Jun 6]. p. 193-206.
- United Nations Office for the Coordination of Humanitarian Affairs (OCHA). Nigeria Situation Report, 17 June, 2023 [Internet]. Geneva (Switzerland): OCHA; 2023 Jun 17 [cited 2024 May 28]; 33p. Download Situation Report - Nigeria - 17 Jun 2023.pdf.
- Ella EE, Ayorinde E, Ameh JB.Comparative seroprevalence of measles virus immunoglobulin M antibodies in children aged 0-8 months and a control population aged 9-23 months presenting with measles-like symptoms in selected hospitals in Kaduna State. IJGM [Internet]. 2015 Mar 10 [cited 2024 May 27];101-10. https://doi.org/10.2147/IJGM.S79423 PubMed | Google Scholar
- Papania M, Baughman AL, Lee S, Cheek JE, Atkinson W, Redd SC, Spitalny K, Finelli L, Markowitz L.Increased susceptibility to measles in infants in the united states. Pediatrics [Internet]. 1999 Nov 1 [cited 2024 May 28];104(5):e59-e5. https://doi.org/10.1542/peds.104.5.e59 Google Scholar
- Nandy R, Handzel T, Zaneidou M, Biey J, Coddy RZ, Perry R, Strebel P, Cairns L.Case-fatality rate during a measles outbreak in eastern Niger in 2003. Clinical infectious diseases [Internet]. 2006 Feb 1 [cited 2024 May 28];42(3):322-8. https://doi.org/1086/499240 Google Scholar
- Muscat M, Ben Mamou M, Shefer A, Jankovic D, Deshevoy S, Butler R.[Situation of measles and rubella in the WHO European Region]. Rev Esp Salud Publica [Internet]. 2015 Aug [cited 2024 May 28];89(4):345-51.https://dx.doi.org/10.4321/S1135-57272015000400002 Spanish.
- Ismail Abdullateef Raji, Auwal Usman Abubakar, Aliyu Mamman Na´uzo, Yahaya Mohammed, Aminu Umar Kaoje, UM Ango.Descriptive Characterisation of Suspected Measles Cases in Sokoto State 2010 -2016: A Secondary Data Analysis. Annals of Basic and Medical Sciences [Internet]. 2021 Jun 30 [cited 2024 May 28];2 (1): 73-78.
- Zheng M, Wang W, Tang M, Zhou J, Boccaletti S, Liu Z.Multiple peaks patterns of epidemic spreading in multi-layer networks. Chaos, Solitons & Fractals [Internet]. 2018 Jan 3 [cited 2024 May 28];107:135-42. https://doi.org/10.1016/j.chaos.2017.12.026 PubMed | Google Scholar
- Omole Victoria Nanben, Musa Emmanuel, Audu Onyemocho, Gajere Julius, Peter Elisha.A Retrospective Investigation of a Measles Outbreak in a District in North-western Nigeria . Public Health International [Internet]. 2017 Jun 8 [cited 2024 Jun 6]2(3): 96-101. https://doi.org/10.11648/j.wjph.20170203.12 Download pdf to view full article. Google Scholar
- WHO. Measles & Rubella surveillance and outbreak investigation guidelines [Internet]. Geneva(Switzerland): WHO; 2009 Jan 1 [cited 2024 May 28]: 99p. Download cover-final.cdr.
- BS Ibrahim, GJ Gana, Y Mohammed , UA Bajoga, AA Olufemi, AS Umar, HB Ayanleke, SO Gidado, AA Abubakar, PM Nguku.Outbreak of measles in Sokoto State North-Western Nigeria, three months after a supplementary immunization campaign: An investigation report 2016. AMJ [Internet]. 2016 [cited 2024 May 28];9(9):324-335. http://doi.org/10.21767AMJ.2016.2697 Download 2697-13941-2-PB.pdf. Google Scholar
- Ori PU, Adebowale A, Umeokonkwo CD, Osigwe U, Balogun MS.Descriptive epidemiology of measles cases in Bauchi State, 2013-2018 . BMC Public Health [Internet]. 2021 Jul 5 [cited 2024 May 28];21(1):1311. https://doi.org/10.1186/s12889-021-11063-6 PubMed | Google Scholar
- Ibrahim M, Jiya NN.Clinical presentation of measles in Sokoto, Nigeria. Sahel Med J [Internet]. 1999[cited 2024 May 28];2(2):104-7. Download pdf to view full article.
- Adesina MA, Olufadewa II, Oladele RI, Solagbade A, Olaoyo C.Determinants of childhood immunization among rural mothers in Nigeria. Popul Med [Internet]. 2023 Sep 15 [cited 2024 May 28];5(September):1-7. https://doi.org/10.18332/popmed/171542 Google Scholar
- Larson HJ, Smith DM, Paterson P, Cumming M, Eckersberger E, Freifeld CC, Ghinai I, Jarrett C, Paushter L, Brownstein JS, Madoff LC.Measuring vaccine confidence: analysis of data obtained by a media surveillance system used to analyse public concerns about vaccines. The Lancet Infectious Diseases [Internet]. 2013 May 13 [cited 2024 May 28];13(7):606-13. https://doi.org/10.1016/S1473-3099(13)70108-7 Google Scholar
- MacDonald NE.Vaccine hesitancy: Definition, scope and determinants. Vaccine [Internet]. 2015 Aug 14 [cited 2024 May 28]; 33(34): 4161-4164. https://doi.org/10.1016/j.vaccine.2015.04.036 Google Scholar
- Brown KF, Kroll JS, Hudson MJ, Ramsay M, Green J, Vincent C A, Fraser G.Factors underlying parental decisions about combination childhood vaccinations including MMR: a systematic review . Vaccine [Internet]. 2010 Jun 11 [cited 2024 May 28]; 28(26): 4235-4248. https://doi.org/10.1016/j.vaccine.2010.04.052 Google Scholar
- Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger JA.Vaccine hesitancy: An overview. Human Vaccines & Immunotherapeutics [Internet]. 2013 Aug 8 [cited 2024 May 28];9(8):1763-73. https://doi.org/10.4161/hv.24657 PubMed | Google Scholar
- Kalil FS, Gemeda DH, Bedaso MH, Wario SK.Measles outbreak investigation in Ginnir district of Bale zone, Oromia region, Southeast Ethiopia, May 2019 . Pan Afr Med J [Internet]. 2020 May 14 [cited 2024 May 28];36: 20. https://doi.org/10.11604/pamj.2020.36.20.21169 PubMed | Google Scholar
- Douangboupha V, Binns P, Khamphaphongphane B, Oulay V, Sengsaiya K, Boupphaphanh T, Xangsayarath P.Factors contributing to a measles outbreak in a hard-to-reach rural village in Xaisomboun Province, Lao People´s Democratic Republic . WPSAR [Internet]. 2022 Aug 3 [cited 2024 May 28];13(3). https://doi.org/10.5365/wpsar.2022.13.3.874 PubMed | Google Scholar
- Minetti A, Hurtado N, Grais RF, Ferrari M.Reaching hard-to-reach individuals: nonselective versus targeted outbreak response vaccination for measles. American Journal of Epidemiology [Internet]. 2014 Oct 16 [cited 2024 May 28];179(2):245-51. https://doi.org/10.1093/aje/kwt236 PubMed | Google Scholar
- Baker M, Mcnicholas A, Garrett N, Jones N, Stewart J, Koberstein V, Lennon D.Household crowding a major risk factor for epidemic meningococcal disease in Auckland children. The Pediatric Infectious Disease Journal [Internet]. 2000 Oct [cited 2024 May 28];19(10):983-90. https://doi.org/10.1097/00006454-200010000-00009 Google Scholar
- Frans Yosep Sitepu, Elpiani Depari, Mudatsir Mudatsir, Harapan Harapan.Being unvaccinated and contact with measles cases as the risk factors of measles outbreak, North Sumatera, Indonesia. Clinical Epidemiology and Global Health [Internet]. 2019 Aug 13 [cited 2024 May 28]; 8(1): 239-243. https://doi.org/10.1016/j.cegh.2019.08.006 Google Scholar
- WHO. Primary Health Care [Internet]. Geneva (Switzerland): WHO; 2023 Nov 15 [cited 2024 May 28].
- Chukwudi, AN, Charles SW, Abdu AA, Maia L, Hassan M, Duduzile N.Missed Opportunities for Vaccination and Associated Factors among Children Attending Primary Health Care Facilities in Cape Town, South Africa: A Pre-Intervention Multilevel Analysis. Vaccines [Internet]. 2022 May 16 [cited 2024 May 28]; 10(5):785. https://doi.org/10.3390/vaccines10050785 PubMed | Google Scholar
- Nuria T, Rubén S, Cristina R, Angela D.Implication of health care personnel in measles transmission . Human Vaccines & Immunotherapeutics [Internet]. 2014 Nov 1 [cited 2024 May 28]; 11(1):288-292. https://doi.org/10.4161/hv.36166 Google Scholar