Characterization of COVID-19 cases in the formal and informal settlements in Dagoretti sub-county Kenya, 2020
Florence Wanjiru Mugo1,&, Ahmed Abade Mohamed1, Peter Kabetu Njenga2, Maurice Owiny1, Fredrick Odhiambo1
1Field Epidemiology Laboratory Training Program, Ministry of Health, Kenya, 2Nairobi Metropolitan Services (NMS), Health Department, Ministry of Health, Kenya
&Corresponding author
Florence Wanjiru Mugo, Field Epidemiology Laboratory Training Program, Ministry of Health, Kenya.
Introduction:
COVID-19 posed a serious public health threat to all ages. In Kenya, it was first detected on March 13, 2020, in its capital - Nairobi, which remained the epicenter of the disease thereafter. Dagoretti is one area that has both formal and informal residencies and showed a marked increase of cases; from a total of nine in March to 1219 in July 2020. The upsurge prompted us to describe the cases as they were being identified through contact tracing.
Methods:
This was a cross-sectional study that involved the review of COVID-19 data from 1st March to 31st July 2020 using a line list. We reviewed data for all COVID-19 cases and their contacts. We generated measures of central tendency for continuous variables and frequencies and proportions for categorical variables.
Results:
Of the 1,620 COVID-19 records analyzed, 98% (1580) had no contact history with a case. The median age was 42 (IQR: 20.5 – 64.5) years. The majority 59.5% (964/1620) were males with 32.7% (529/1620) from the age group of 31-40 years. The formal settlements had higher infections at 85.7% (1,389/1,620). All 16 deaths (100%) were from formal residencies out of which 62.5% (10/16) had comorbidities.
Conclusion:
COVID-19 disproportionately affected the formal dwellers in the early days of the pandemic. The highest mortality occurred in cases with comorbidities. We recommended targeted advocacy and scale-up of COVID-19 awareness to diabetic and hypertensive cases in both residencies.
Introduction

The first case of COVID-19 in Kenya was confirmed on March 13, 2020, in the capital city, Nairobi [1]. The total number of confirmed cases in Kenya as of August 15, 2020, was 29,849 cases and 472 deaths (CFR=1.6%). Of these, 29,271 cases (98%) were local transmissions and 578 (2%) were imported cases. The majority of the confirmed cases, at 27,874 (93 %) were asymptomatic [2].
During the early days of COVID-19 in Africa, the disease was majorly imported and from the formal dwellers [
3]. This could have been due to international travel associated with affluence. As the outbreak continued, it started spreading among the informal dwellers which could have been caused by the poor observance of COVID-19 measures as recommended by the World Health Organization (WHO) including observance of at least 1-meter social distance; hand washing with soap and water or alcohol-based liquids; wearing of masks; movement restriction among the informal residents as a result of overcrowding, lack of water, sanitation, and hygiene amenities in the informal settlements [
4,
5].
Contact tracing, active case search were key in identifying COVID-19 cases to contain the spread of the disease in different parts of the world [
6]. At the time, the Government of Kenya had given a directive to conduct targeted testing to prevent transmission and slow the spread of SARs CoV-2. The Case Investigation Forms (CIF) were filled at the point of sample collection and it captured most of the biodata of the suspected cases. Kenya adopted contact tracing as one of the strategies and as of July 30, 2020, a total of 19,913 confirmed cases of COVID-19 had been reported. By this time, 17,488 contacts had been listed with 14, 696 (74%) contacts not listed. The overwhelming workload of contact tracing for healthcare workers, misinformation in the population, stigma, and wanting to isolation and quarantine measures lead to contacts not being listed [
7].
Nairobi is the capital city of Kenya and was the epicenter of COVID-19 infections. The County (sub-national) government of Nairobi had reported the highest attack rate of 269.2 per 100,000 population for COVID-19, compared to the national attack rate of 41.9 per 100,000 population as of July 30, 2020 [
8]. Dagoretti is a populous area in Nairobi, that has both formal and informal residencies and was a hotspot for COVID-19 [
9]. Some of the published studies in the early days of the pandemic had focused on the characterization of cases in the formal and informal settlements and on the impact of COVID-19 control measures in such settings [
4,
10,
11]. None of these studies compared contact tracing between the two settlements. Dagoretti had reports of increased COVID-19 cases from a total of nine in March to 1,219 in July 2020 as of the time of this study. The Ministry of Health, through the National Emergency Operation Center (EOC), dispatched a Rapid Response Team (RRT) mandated with contact tracing to conduct an active case search for COVID-19. We described COVID-19 cases as they were being identified through contact tracing in the Dagoretti area of Nairobi, Kenya.
Methods

Study area
Dagoretti is located in Nairobi Subnational and the capital city of Kenya hosting approximately 432,331 people with a population density of 14,908 per km
2. Dagoretti area is divided into 10 wards among which Kileleshwa and Kilimani wards are considered to be the formal residence for high-income earners including expatriates while Kawangware ward which is adjacent to both Kileleshwa and Kilimani wards is densely populated and considered informal. The other seven wards were informal and had reported a smaller number of COVID-19 cases at the time of the study. According to the United Nations Human Settlement definition, formal settlements are designed and developed to offer basic services to their residents and have formal recognition or approval from the government authorities while informal settlements are characterized by poverty and poor access to basic services, improper building structures, unhealthy and dangerous environmental conditions, unsafe residency rights, and social deprivation [
12]. Some of the residents from Kawangware seek daily casual labour in Kileleshwa and Kilimani wards and others stay as domestic servants in the affluent wards.
Study design
This was a cross-sectional study that involved the review of COVID-19 data from August 10, 2020, through August 15, 2020. We reviewed data for all COVID-19 cases and their contacts.
Data collection
Data were abstracted from the COVID-19 Case Investigation Form (CIF) at the National Public Health Laboratory and Kenya Medical Research Institute (KEMRI) laboratories. The variables collected included demographic characteristics: age (years), sex, area of residence; travel history (prior 14 days), history of contact with COVID-19 case, co-morbidities, date of laboratory confirmation, signs and symptoms, and case outcomes (Alive or Dead). We called all the cases to generate the list of their contact through snowballing and used the data to generate a transmission chain. If there was no contact linked to a case, the chain was completed at that point. Where the data on stated variables were missing in the CIF we contacted the cases through a phone call to update the line list. In scenarios where this was not possible or the case was dead, we contacted their next of kin.
Laboratory confirmation was by Reverse Transcription Polymerase Chain Reaction (RT-PCR) from March 1, 2020, to July 30, 2020, in the Dagoretti area [
13]. A respondent with an incorrect telephone number or who did not disclose their COVID-19 test status was excluded from the line listing.
Data management and analysis
We analyzed data using Epi Info 7 (Center for Disease Control and Prevention, Atlanta, GA, USA). We generated measures of central tendency for continuous variables and frequencies and proportions for categorical variables.
Ethical Considerations
To ensure confidentiality, verbal consent was requested from cases and patients' records were de-identified using codes. The data were stored in a password-protected database on a personal computer with access limited to the lead investigators.
Results
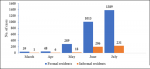
A total of 1632 records of COVID-19 cases were reviewed of which 99.3% (1,620/1,632) were analyzed. In March 2020, there were 0.5% (8/1,620) cases from the formal settlement and 0.1% (1/1,620) case from the informal settlement while in July of the same year, the cases had increased to 63% (1,013/1,620) in the formal and 13% (206/1,620) cases in the informal residencies. A peak of the cases was recorded in July (Figure 1 and Figure 2). Majority of the cases were male 59.5% (964/1,620). In both sexes, the majority of the cases were from the formal settlement at 39.4% (547/1,389) female and 60.6% (842/1,389) male respectively (Table 1). At the initial stages of COVID-19 in March 2020, nearly 78 % (7/9) of the cases had a history of contact with a confirmed COVID-19 case. Of all the cases by the end of July, 97.5% (1,580/1,620) had no contact history with a COVID-19 case.
The median age was 42 (IQR: 20.5-64.5) years, with the age band of 31-40 years contributing the highest number of cases 32.7% (529/1,620) followed by 21-30 age band at 24.0% (388/1,620). Only 2% (35/1,620) had travelled as an exposure and they were all from the formal residents. There was a disparity in both residencies where the formal residencies had the highest infections at 85.6% (1,389/1,620) with an attack rate of 52 per 10000 population.
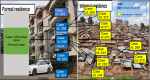
The first case in Dagoretti was an employee of an international organization residing in a formal settlement and working as a volunteer in contact tracing at the national level in the Ministry of Health. The case was diagnosed during mass testing that targeted all healthcare workers. A total of 14 contacts were linked to the case. Out of the 14 contacts, one was a nanny residing in the informal settlement and working as a day-based house help for this case. The nanny was later linked to four more cases residing in the informal residencies while a friend to the index case was linked to five cases in the informal settlement (
Figure 3).
Of all the cases, only 12.1% (196/1,620) were symptomatic with cough 5.3% (86/1,620) being the most common of the symptoms (
Table 2). A total of 70 (4.3%) cases had comorbidities (
Table 2). Hypertension at 1.2% (19/1,620), Asthma at 0.7% (11/1,620), Diabetes at 0.6% (9/1,620) and Diabetes combined with hypertension at 0.6% (9/1,620) were the major comorbidities recorded at a total of 2.3% (48/1,620). The proportion that had other comorbidities (cancer of the tongue; chronic kidney disease; multiple myeloma; pulmonary tuberculosis; cardiovascular diseases) was at 1.4% (22/1,620) of the cases. There was a disproportionate distribution of the comorbidities by residence with 4.8% (67/1,389) among formal residents compared to 1.3% (3/231) among the informal residents. Forty (2.5%) of the 1620 cases that had comorbidities were males while 30 (1.9%) were females. More males than females had hypertension (10 male, 9 female), diabetes (8 male, 1 female), and other comorbidities (12 male, 10 female) while the reverse was true for asthma (male 4, female 7). The other comorbidities included cancer of the tongue, chronic kidney disease, multiple myeloma and pulmonary tuberculosis.
All deaths 16 (100%) were from the formal settlement and the overall case fatality rate (CFR) was 0.99% (16/1,620). Among the deaths, 62.5% (10/16) had comorbidities (
Table 3) contributing to 0.6% (10/1,620) of the deaths among all cases. Of the deaths, 75% (12/16) occurred among those aged 50 years and above, the remaining 25% of deaths occurred among the age group 31-40 years (2/16) and 41-50 years (2/16).
Discussion
Our data review from the contacts tracing exercise indicated that there was a disparity in COVID-19 caseload in the early days which could have been due to lifestyle that included international travels associated with the affluence. Air travel contributed to the worldwide spread of COVID-19 hence accelerating transmissions between countries. Kenya suspended its international flights to and from the Country on March 23, 2020, and only cargo flights were allowed to operate while the crew was supposed to strictly observe the COVID-19 measures. All individuals getting into the Country were immediately quarantined for fourteen days at their cost. There was also evidence of community transmission between the formal and informal settlements, where the index case was from the formal settlement and working with an international organization could have exposed the case to COVID-19. The place of work, mode of work, duration of contact, and mode of transport were found to influence the transmission of infectious diseases, especially in urban dwellings. The interaction of the domestic worker with the family in the formal settlement where she worked during the day and with the community where she resided may have contributed to the spread of the virus from the formal settlement to the informal settlement. Some of the containment measures instituted by the government of Kenya were limiting the movement of people in the affected areas, however, this did not apply to employees considered as essential workers. Some employees, like domestic workers, could have taken advantage of this provision to continue moving from formal to informal settlements and vice versa. It would be advisable to have domestic employees working in peoples´ homes be housed within the home where they are working to reduce transmissions of infectious diseases during outbreaks.
From the cases description, the male gender contributed to the majority of the cases compared to the females. Findings from studies on why men are more vulnerable to COVID-19 than women relate this to either behavioral or lifestyle factors such as men having a higher tendency to smoke and drink alcohol compared to women; women having a responsible attitude toward the COVID-19 pandemic; irresponsible attitude among men reversibly affecting their undertaking of preventive measures such as frequent hand washing, wearing of face mask, and stay at home orders. During pandemics and other stressful public health events, people tend to engage in stress-relieving activities like smoking cigarettes and drinking alcohol in social places hence posing a higher risk. An investigation carried out in Germany on the effects of COVID-19 during lockdown concluded that the adult population increased their alcohol consumption and smoking as a result of subjective stress due to the COVID-19 pandemic. Another study conducted in China was on the contrary and found out that alcohol consumption had declined in China compared to pre COVID-19 consumption. However, it was consistent with other findings that the male gender contributed the highest proportion among alcohol consumers. This scenario may have been witnessed in the informal settlement where rates of unemployment could be high with the people, mostly men, having more time to meet in social places to pass time.
The age group that contributed the majority of the cases was the 31-40 years´ old who are expected to be in employment or have young families to be fended for. This was in tandem with a study conducted in Nigeria that showed that COVID-19 infection was high among this age group. This age group could be made of people who stay out of their houses for long periods either for work-related activities or social gatherings. Studies have shown that staying out of houses for a long period may predispose an individual to the transmission of COVID-19, especially in areas with high population density as seen in most informal settlements. A study done in Nairobi slums also concluded that the main reason for mobility was employment and job hunting.
Symptomatic cases were less among all the cases, with cough being the most predominant symptom followed by fever and difficulty in breathing. This was consistent with a study that concluded that the most occurring symptoms in COVID-19 are fever, breathing difficulty, malaise, dry cough, and chest pain. All deaths (100%) occurred from the formal settlement with a Case Fatality Rate of CFR=0.99% (16/1,620). Most deaths occurred in the age group 50-60 and among the deaths, the majority had hypertension, diabetes and asthma as the dominant comorbidities. Old age and the presence of co-morbidities may also be associated with developing the severe disease. Diabetes and hypertension formed the highest proportion of the comorbidities. This could have increased the risk of death among the cases, since majority of the cases that died had either of the two comorbidities. Other studies indicated that patient-related outcomes are likely to be worse if there are associated comorbidities.
Another study on COVID-19 and comorbidities concluded that a population with pneumonia-like symptoms and patients with other comorbidities were utmost at risk of infection while individuals with hypertension and diabetes among other comorbidities could develop severe disease and contribute to mortality. Contrary to this study, none of the cases with asthma from our sample died. This could have been a result of proper management of the asthma rather than the severity of the disease. This finding was in concurrence with other studies conducted United Kingdom that suggested that poorly controlled asthma is a risk factor for severe COVID-19 [
14,
15].
This review further highlights the importance of effective contact tracing where we were able to contact trace the index case that may have been implicated in the transmission of the disease to fourteen people. The primary contact who was a domestic worker working for the index case may have acted as the main spreader of the disease from the formal to the informal residents. The further spread in informal settlements could have escalated faster than in the formal setup as a result of overcrowding, poor water, sanitation, and hygiene (WASH) amenities [
6,
7].
The findings in this report are subject to some limitations. Some variables had missing information and this may have led to an underestimation of the figures. Death was taken as recorded in the CIF and confirmed verbally in case a call went through thus no verifiable document was used. Nevertheless, we sought additional information from the cases whose telephone contacts were available. The inadequate testing logistics, stressed contact tracing and other COVID-19 response interventions could have contributed to undetected COVID-19 community spread especially in the informal settlements. The Epicurve was generated from the date of laboratory confirmation of COVID-19.
Conclusion
Contact tracing exercise indicated that there was evidence of community transmission between the formal and informal settlements. COVID-19 disproportionately affected the formal dwellers with mortality being highest among those with hypertension and diabetes comorbidities. Community transmission could have been the major contributor to the rising number of cases as a result of interactions between the formal and the informal dwellers as the informal dwellers partake the manual work in the formal residencies. We recommended targeted and integrated isolation rooms for diabetic and hypertensive cases, continued involvement of a multidisciplinary team in the management of COVID-19 cases with co-morbidities; scale-up COVID-19 education to diabetic and hypertensive cases, and continued enforcement of COVID-19 containment measures to curb community transmission.
What is known about this topic
- COVID-19 signs and symptoms
- COVID-19 prevention and control measures
What this study adds
- New evidence on the disproportionate disparity in COVID-19 caseload in the early eras
- Patterns of COVID-19 transmission between the formal and informal settlements
- New knowledge on workplace exposure to COVID-19
Competing interests
The authors declare no competing interests.
Authors' contributions
Florence Wanjiru Mugo: Conceptualized the original idea of the research, conducted the data analysis, drafted the zero draft of the manuscript, addressed all the reviewer's comments, proofread and fine-tuned the manuscript. Peter Kabetu Njenga: Approved the original idea of the research, assisted in data collection and cleaning. Ahmed Abade Mohamed: Assisted in initial data analysis and proofread the zero draft manuscript. Fredrick Odhiambo: Conceptualized the original idea of the research, oversaw the entire process including its planning, execution, and manuscript preparation, revised the zero draft manuscript for intellectual content, clarity, and accuracy, assisted in addressing all the reviewer's comments. Maurice Owiny: Revised the zero draft manuscript for intellectual content, clarity, and accuracy, oversaw manuscript preparation and execution, assisted in addressing all the reviewer's comments and fine-tuning the manuscript.
Acknowledgments
We would like to thank the following organizations for supporting the investigation: The Division of Disease Surveillance and Response - Kenya; Kenya Field Epidemiology Training Program; Nairobi Metropolitan Services.
Tables and figures
Table 1: Characteristics of the COVID-19 cases in Dagoretti sub-counties, March to July 2020
Table 2: Clinical Characteristics of the COVID-19 Cases in Dagoretti Area, March - July 2020
Table 3: COVID-19 cases characteristics by their outcome in Dagoretti Area, March - July 2020
Figure 1: Distribution of COVID-19 cases March-July, 2020 in Dagoretti Sub County, Kenya
Figure 2: Dagoretti COVID-19 caseloads from March to July 2020
Figure 3: A case scenario of formal to the informal settlement transmission chain
References
- Ministry of Health (KE). COVID-19 outbreak in Kenya Daily Situation Report -002. Nairobi (Kenya): Ministry of Health; 2020 Mar 18. 5 p.
- World Health Organization. Coronavirus disease (COVID-19) Situation Report- 208 [Internet]. Geneva (Switzerland): World Health Organization; 2020 Aug 15 [cited 2024 April 9]: 16 p. Download 20200815-covid-19-sitrep-208.pdf by clicking on download button.
- World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report - 55 [Internet]. Geneva (Switzerland): World Health Organization; 2020 Mar 15 [cited 2024 April 9]:[about 9 pages]. Download 20200315-sitrep-55-covid-19.pdf.
- Corburn J, Vlahov D, Mberu B, Riley L, Caiaffa WT, Rashid SF, Ko A, Patel S, Jukur S, Martínez-Herrera E, Jayasinghe S, Agarwal S, Nguendo-Yongsi B, Weru J, Ouma S, Edmundo K, Oni T, Ayad H.Slum health: arresting covid-19 and improving well-being in urban informal settlements . J Urban Health [Internet]. 2020 April 24 [cited 2024 Apr 9];97(3):348-57. https://doi.org/10.1007/s11524-020-00438-6 Google Scholar
- Von Seidlein L, Alabaster G, Deen J, Knudsen J.Crowding has consequences: Prevention and management of COVID-19 in informal urban settlements . Building and Environment [Internet]. 2020 Nov 22 [version of record 2021 Jan 15; cited 2024 Apr 9];188:107472. https://doi.org/10.1016/j.buildenv.2020.107472 PubMed | Google Scholar
- Aleta A, Martín-Corral D, Pastore Y Piontti A, Ajelli M, Litvinova M, Chinazzi M, Dean NE, Halloran ME, Longini Jr IM, Merler S, Pentland A, Vespignani A, Moro E, Moreno Y.Modelling the impact of testing, contact tracing and household quarantine on second waves of COVID-19 . Nat Hum Behav [Internet]. 2020 Aug 5 [cited 2024 Apr 9];4(9):964-71. https://doi.org/10.1038/s41562-020-0931-9 PubMed | Google Scholar
- Nachega JB, Atteh R, Ihekweazu C, Sam-Agudu NA, Adejumo P, Nsanzimana S, Rwagasore E, Condo J, Paleker M, Mahomed H, Suleman F, Ario AR, Kiguli-Malwadde E, Omaswa FG, Sewankambo NK, Viboud C, Reid MJA, Zumla A, Kilmarx PH. Contact tracing and the covid-19 response in Africa: best practices, key challenges, and lessons learned from nigeria, rwanda, south africa, and uganda . The American Journal of Tropical Medicine and Hygiene [Internet]. 2021 Feb 11 [cited 2024 Apr 9];104(4):1179-8. https://doi.org/10.4269/ajtmh.21-0033 PubMed | Google Scholar
- Ministry of Health (KE). COVID-19 outbreak in KENYA daily situation report - 117. Nairobi (Kenya): Ministry of Health (KE); 2020 July 12. 14 p.
- Ministry of Health (KE). Summary COVID-19 pandemic situation report (SITREP) Number 23: (cases, deaths, transmission scenario). Nairobi (Kenya): Ministry of Health (KE); 2020 July 16. 7 p. Joint publication of the Nairobi Metropolitan Services.
- Quaife M, Van Zandvoort K, Gimma A, Shah K, McCreesh N, Prem K, Barasa E, Mwanga D, Kangwana B, Pinchoff J, CMMID COVID-19 Working Group, Bosse NI, Medley G, O´Reilly K, Leclerc QJ, Jit M, Lowe R, Davies NG, Deol AK, Knight GM, Auzenbergs M, Edmunds WJ, Atkins KE, Jombart T, Eggo RM, Foss AM, Flasche S, Pearson CAB, Nightingale ES, Munday JD, Abbott S, Quilty BJ, Gibbs HP, Simons D, Emery JC, Hué S, Liu Y, Tully DC, Rosello A, Procter SR, Endo A, Russell TW, Rees EM, Diamond C, Meakin SR, Kucharski AJ, Gore-Langton GR, Klepac P, Hellewell J, Sun FY, Houben RMGJ, Villabona-Arenas CJ, Funk S, Clifford S, Brady O, Edmunds WJ, Jarvis CI, Austrian K.The impact of COVID-19 control measures on social contacts and transmission in Kenyan informal settlements . BMC Med [Internet]. 2020 Oct 5 [cited 2024 Apr 9];18(1):316. https://doi.org/1186/s12916-020-01779-4 PubMed | Google Scholar
- Parikh P, Diep L, Gupte J, Lakhanpaul M.COVID-19 challenges and WASH in informal settlements: Integrated action supported by the sustainable development goals. Cities [Internet]. 2020 Sep 8 [cited 2024 Apr 9];107:102871. https://doi.org/10.1016/j.cities.2020.102871 PubMed | Google Scholar
- Ghasempour A.Informal Settlement; Concept, Challenges and Intervention Approaches. Spec J Archit Constr [Internet]. 2015 [cited 2024 Apr 9];1(3):10-6. Google Scholar
- Ministry of Health (KE). Targeted testing strategy for COVID-19 in Kenya [Internet]. Nairobi (Kenya): Ministry of Health (KE); 2020 [cited 2024 Apr 9]; p. 1-63.
- Bloom CI. Covid–19 pandemic and asthma: What did we learn? Respirology [Internet]. 2023 May 8 [cited 2024 Apr 9];28(7):603-14. https://doi.org/10.1111/resp.14515 Google Scholar
- Franco PA, Jezler S, Cruz AA.Is asthma a risk factor for coronavirus disease-2019 worse outcomes? The answer is no, but … . Current Opinion in Allergy & Clinical Immunology [Internet]. 2021 Jan 29 [cited 2024 Apr 9];21(3):223-8. https://doi.org/10.1097/aci.0000000000000734 Google Scholar