COVID-19 outbreak investigation among construction workers at a construction site in Harare, Zimbabwe February - March 2021
Amanda Sarah Thakataka1, Joseph Mberikunashe2, Emmanuel Govha1, Tsitsi Patience Juru1,&, Notion Tafara Gombe3, Mufuta Tshimanga1
1Department of Primary Health Care Sciences, Family Medicine, Global and Public Health Unit, University of Zimbabwe, Harare, Zimbabwe, 2National Malaria Control Program, Ministry of Health and Child Care, Harare, Zimbabwe, 3African Field Epidemiology Network, Harare, Zimbabwe
&Corresponding author
Tsitsi Patience Juru, Zimbabwe Field Epidemiology Training Programme, 3-62 Kaguvi Building, Corner 4th/Central Avenue, Harare, Zimbabwe. tsitsijuru@gmail.com
Introduction:
On February 16, 2021, a construction site in Harare recorded 26 COVID-19 cases during routine worker screening. Over five days, the positivity rate increased from 4.14 to 7.29%. Workplace outbreaks affect productivity. We investigated the outbreak among construction workers to determine the workplace factors associated with contracting COVID-19.
Methods:
We verified the outbreak, carried out an environmental assessment, line-listed the positive workers, and assessed the emergency preparedness and response. A retrospective cohort study was done. We recruited 150 workers from all 700 construction workers, obtained written consent and used self-administered questionnaires to collect data. Epi Info 7.2.4.0™ was used for data capturing and analysis. We conducted a univariate, bivariate and multivariate analysis using forward stepwise logistic regression to determine the independent factors. An Epi-curve was constructed using Epi Info and a spot map using Lucid Chart software.
Results:
The response was timely but inadequate. There was overcrowding with a sleeping space area of 1.43m2/individual against a minimum requirement of 3.5 m2/individual. Out of 150, 76 (51%) tested positive, most being male, 106/150 (71%). Independent risk factors were smoking >20 cigarettes/day (aRR=8.42; 95% CI 2.02-35.10) and sharing bathrooms and toilets with >50 people (aRR=4.28; 95% CI 1.27-14.4). Owning a hand sanitiser (aRR=0.20; 95% CI 0.06-0.67) and prior vaccination (aRR=0.16; 95% CI 0.05-0.48) were protective factors.
Conclusion:
Overcrowding resulted in poor hygiene and shared facilities propagated the outbreak. The benefit of preventive behaviour and COVID-19 vaccination was shown. We recommended for enforcement of infection prevention measures and the reduction of exposures in the workplace.
Introduction

Coronavirus-2019 Disease (COVID-19) is a respiratory tract disease caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) [1,2]. COVID-19 is transmitted from person to person even in the asymptomatic phase through respiratory droplets when an infected person coughs, sneezes or comes into contact with contaminated surfaces [3]. The common clinical symptoms are fever, dry cough, shortness of breath and tiredness. Diarrhoea, gastrointestinal upset, sore throat, sneezing and nasal congestion are other reported symptoms. Eighty percent of infected individuals tend to have mild asymptomatic disease, the rest will have overt signs and symptoms with some requiring hospital admission [2,4]. Host susceptibility to infection and severity of symptoms have been described as determinants of progression to COVID-19 [3,5].
COVID-19 was declared a global pandemic on March 11, 2020, after a cluster of cases of pneumonia of unknown cause had been reported from Wuhan, a city in China in December 2019 [
6,
7]. Zimbabwe mimicked the rest of the world at the events surrounding the pandemic. After the country´s first case on March 20, 2020, the first nationwide lockdown was sanctioned. During this lockdown, emergency epidemic preparedness was intensive [
8]. The setting of the 9 pillared Emergency Response Plan chaired by the Secretary for Health and a high-level inter-ministerial task force directed by the presidential office was to guide the National COVID-19 response. The lockdown restrictions saw the shutting down of schools and businesses deemed unessential, shorter business operating times and travel restrictions between and within cities and towns [
9,
10]. The country´s warnings for a possible 2
nd wave in the last quarter of 2020 were taken with much complacency. By December 2020 the second wave had hit the country. Controlling for this was almost a futile exercise, with the burden of hospitalisations overtaking events [
11]. On February 14, 2021, Zimbabwe had reported 30 601 cases of COVID-19 and 1400 deaths [
12].
On February 16, 2021, a construction site in Mount Hampden manned by Chinese nationals recorded 26 SARS-Cov-2 positive workers during routine screening. Over the proceeding 5 days, 203 of the 700 workers had tested positive and none of the workers had reported signs and symptoms of COVID-19. Those who tested positive were immediately sent for isolation at a different facility. The daily positivity rate rose from 4.14 to 7.29% in a week. When routine screening was complete, the company was operating at a reduced capacity with almost 30% of workers in isolation. Workplace outbreaks affect productivity, because the policy for field-based work like construction work, was to conduct routine COVID-19 screening, isolate positive workers and quarantine contacts. We investigated the COVID-19 outbreak among construction workers to determine the workplace factors associated with contracting COVID-19. We also assessed the COVID-19 epidemic preparedness and response of the district health team.
Methods

Epidemiological Investigation
We verified the COVID-19 outbreak by performing Reverse-Transcription Polymerase Chain Reaction (RT-PCR) for SARS-Cov-2 from nasopharyngeal swabs among the construction site workers. All 700 workers were tested. Contacts were defined as people who lived and worked together in the same place or within one-metre distance with a confirmed case for a period longer than 15 minutes. A confirmed COVID-19 case was defined as a person with an RT-PCR positive result. We defined a suspected case of COVID-19 as any worker at the site who was present at the site from 14 days before the routine testing commenced. Any person working with a confirmed case within 14 days was considered a suspect [
13]. We identified the cases using these case definitions. A line list with demographic information and disease outcomes was created for the confirmed cases. From the preliminary descriptive epidemiology, we hypothesized that there was no association between sharing a sleeping space and contracting COVID-19 among construction workers at Mount Hampden in 2021.
Study Design
We conducted a retrospective cohort study to test our hypothesis. The population under investigation was well-defined and shared a common workplace. We chose this design because it is quick to conduct as both the exposure and outcome had occurred.
Study Setting
Mount Hampden is a new capital city under construction, located on the outskirts of Harare. A Chinese private developer was contracted at one site, for the construction of the new parliament which was set to be completed in March 2021. This target was not met because of COVID-19-related delays, lockdowns and slow movement of materials needed for construction. Routine COVID-19 screening of workers was mandated by the government and enforced through a statutory instrument by the task force [
14]. The workers at this site were Chinese citizens with government medical insurance and their medical care was arranged through the Chinese Ambassador.
Study Population
The study population was construction workers of Asian origin living and working at the construction site.
Inclusion Criteria: Any worker who was tested for COVID-19 between 16 and 20 February 2021 using RT-PCR and consented to participate in the study was included.
Exclusion Criteria: Workers who were admitted due to illness were excluded from the study. Seeking approval to access those in a healthcare institution would have been time-consuming. Eight cases were admitted to the hospital and excluded from the study.
Sample Size Determination and Sampling
A minimum sample size of 105 was calculated using the StatCalc function embedded in Epi Info 7 (CDC, 2019). This was based on a study by Ng et al., 2020 where an association between sharing a bedroom and a toilet with a COVID-19 case was independently associated with contracting the infection. A proportion of 50.6% in the exposed and 21.4% in the unexposed, OR of 10.62 (95% CI 5.84-19.33) was used [
15]. We assumed a 95% CI, 80% power and 10% attrition rate. Simple random sampling was used to select 150 participants from a list of the 700 workers at the construction site. A calculated sample size was used all 700 workers could not be recruited into the study because of time and other resource constraints. A simple random selection of numbers from this list was done using random numbers generated by Microsoft Excel. We enrolled more participants to increase confidence in our estimates and have greater precision in the results.
Data Collection Tools and Techniques
A pretested self-administered questionnaire was used to collect data. The questionnaire was translated from English to a formal modern Chinese dialect by a hired translator. The translations were verified by a Chinese medical practitioner for clarity of medical terminology. To pre-test the questionnaire, 11 Chinese workers completed the questionnaire in the presence of the principal investigator, the translator and the medical practitioner. These represented 10% of anticipated study participants and were excluded from the study. Corrections were made on areas that needed clarity.
The outcome variable in this study was having tested positive for COVID-19 (i.e. having the disease). The risk factors potentially attributable to being infected with COVID-19 were then compared between the diseased and those who did not have the disease (i.e. those testing negative for COVID-19). Demographic information, risk factors for contracting COVID-19 based on participants´ responses, underlying illnesses, presence of signs and symptoms of COVID-19 and COVID-19 vaccination. An assessment of outbreak preparedness and response for Zvimba District was done using a checklist created based on the Integrated Disease Surveillance and Response (IDSR) Technical Guidelines [
16]. The checklist assessed the district´s response time, and the adequacy of the team responding to the outbreak in terms of decision-making capacity and technical ability to make decisions. An environmental assessment was done using a checklist. We toured the living and working areas and observed the use of COVID-19 prevention protocols. We collected information on the number of inhabitants per living space and measured the sleeping spaces to determine the average space utilized by each worker in the living quarters. Sleeping space was defined as the barrack in which a person regularly sleeps at night.
Data Analysis
Data were captured and analysed using Epi Info 7.2.4.0™(CDC, 2020) statistical software to generate means, frequencies, proportions, and attack rates. Bivariate analysis was done to analyse the relationship between the outcome variable and the risk factors to ascertain if any associations were present. Multiple exposures were computed against the outcome variable and relative risks, their 95% confidence intervals and p-values were generated. Multivariate analysis was done to determine the independent factors of contracting COVID-19, using forward stepwise logistic regression. All variables with a chi-square p-value ≤0.25 were included in the model. We chose p-value ≤0.25 as the threshold for including variables in the multivariate model because this has been suggested elsewhere as an appropriate threshold [
17]. Measures of impact were computed for the independent risk factors, Attributable risk (AR), population attributable risk (PAR), AR% and PAR%.
Ethical Considerations
Approval to conduct the study was obtained from the Ministry of Health and Child Care through the District Medical Officer (DMO) for Zvimba District and the Health Studies Office (HSO). These institutions reviewed the protocol and approved the study to proceed. Permission to engage workers was sought from the company management and the isolation facilities. Informed written consent was obtained and confidentiality was assured by excluding names during data collection. Privacy was maintained during the interviews by individualising the sessions. It was communicated that participation was voluntary, and participants could withdraw at any point in time during the study. COVID-19 prevention and control regulations were observed.
Results
Descriptive Epidemiology
Outbreak description by person
The total number of workers tested was 700 and 203 workers tested positive for COVID-19 between 16-20 February 2021. The overall positivity rate was 29%. We recruited 150/700 workers into the study, 76/150 (51%) were positive cases. Most of the positive cases were male, 64/76 (84%). The median age of cases was 39.5 years (Q
1=34.5; Q
3= 46.5), and most were above 35 years, 57/76 (75%). Among the 76 who tested positive, 4/76 (5%) were asymptomatic at the time of testing. The most common symptoms were myalgia 37/76 (49%), sneezing and sore throat reported by 26/76 (34%) of cases. All 76 cases received basic treatment for COVID-19 with Vitamin C 500mg and Zinc Sulphate supplements daily plus Azithromycin antibiotic for those who reported symptoms, 72/76 (95%).
Outbreak Description by Place
The highest attack rate was among the workers who lived in Staff Barracks D, 78% and C, 61%. These barracks were located within the same boundary and shared an eating area. Similarly, staff barracks B and A were in the same boundary and shared an eating area; their attack rates were 56% and 48% respectively. Staff barrack E had an attack rate of 33%, this is the barrack that housed the female workers. The quarantine barrack had an attack rate of 25% (
Figure 1).
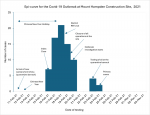
Description of the Outbreak by Time
The first diagnosed case was on February 16, 2021. The primary cases were diagnosed on February 23 and 24, 2021, these were new workers from China who had arrived on February 11, 2021, to start working after a 14-day quarantine period. They broke their quarantine and interacted with other workers during Chinese New Year celebrations which begun on February 11 to 17. The Chinese New Year was on February 12, 2021. They did not get tested on arrival and had no symptoms. The celebration is a festival of drinking, feasting, and playing games which were done in the largest compound housing the barracks we named C and D.
Positive cases were sent to a private isolation facility. The local health officials were informed of these cases the next day (February 17, 2021) as testing continued. The Rapid Response Team (RRT) visited the site on February 18, 2021, leading to the closure of the site the next day and subsequent testing of the remaining workers. Control measures were put in place, which included halting operations at the site, disinfection of premises, isolation of cases and quarantine of the rest of the workers in controlled environments. The outbreak was declared over on March 31, 2021, after 2 cycles of 2 weekly tests on all workers and construction operations resumed on April 5, 2021. The Epi-curve showed a point source mode of spread (
Figure 2).
Epidemic preparedness, response and Environmental Assessment
The RRT visited the site within 24 hours of the outbreak being reported. This was a timely initial response. The RRT was adequately composed of key personnel, the DMO, environmental health officer, laboratory scientist and local environmental health technician. The company had contracted a private laboratory to conduct the COVID-19 tests. The RRT gave guidance on quarantine procedures and testing of workers. To ensure this guidance was adhered to and monitor adherence to control measures the RRT conducted two follow-up visits for the environmental assessment of the work area, living quarters to check on the improvements in the work area for infection control and prevention. The initial checklist for environmental assessment was used for the follow-up visits.
The working areas were clean and most work was done outdoors. There was poor screening at entry points as no temperature checks were done at entrances and no hand hygiene points were seen in the work area. In the living areas, we noted poor ventilation, as the containerised houses had makeshift window openings. The living spaces were dirty and there was poor sanitation in the washrooms. There was overcrowding in the worker´s sleeping spaces, with an area of 1.43 m
2 per individual against a minimum requirement of 3.5 m
2 per person by United Nations High Commissioner for Refugees (UNHCR) standards for emergency/temporary [
18]. Dining areas were well maintained, clean and there were handwashing points. There was poor social distancing with workers scrambling at the canteen during mealtimes.
Analytical Epidemiology
Demographic characteristics of study participants
Most of the participants were male, 110/150 (73%). The median age was 37 years (Q1=32; Q3=45), with most 101/150 (67%) being older than 35 years. Most participants were engineers, 24/150 (16%). The most prevalent underlying illness was hypertension, 40/150 (27%) (
Table 1). The COVID-19 attack rate was higher in males 58% (64/110) and among those above 35 years of age 56% (57/101) .
Bivariate Analysis
Statistically significant risk factors were being male (RR 1.93; 95% CI 1.17 - 3.19), age above 35 years (RR 1.46; 95% CI 1.05-2.02), having asthma (RR 1.65; 95% CI 1.16-2.35) and hypertension (RR 1.43; 95% CI 1.05-1.94). Smoking was a risk factor (RR 1.77; 95% CI 1.19-2.61), sharing cigarettes (RR 1.72; 95% CI 1.25 - 2.36) and smoking ≥20 cigarettes/day (RR 1.68; 95% CI 1.26 - 2.23) were all significantly associated with contracting COVID-19. Sharing eating utensils (RR 1.74; 95% CI 1.29-2.34), a sleeping space with ≥10 people (RR 1.62; 95% CI 1.16-2.25), bathrooms and toilets with ≥50 people (RR 1.67; 95% CI 1.24-2.21) and eating in common eating areas (RR 1.60; 95%CI: 1.47-2.66) were also significant risk factors.
Consistent face mask use (RR 0.52; 95%CI: 0.39-0.69) and face mask use during meetings and gatherings (RR 0.59; 95%CI: 0.40-0.88) were significant protective factors. Access to a handwashing facility (RR 0.56; 95%CI 0.42-0.75), consistent handwashing with soap (RR 0.31; 95% CI 0.17-0.57), owning a hand sanitiser (RR 0.46; 95%CI: 0.34-0.62) and frequent use of hand sanitisers (RR 0.45; 95% CI 0.24-0.84) were significant protective factors against COVID-19. Being vaccinated for COVID-19 was protective against contracting COVID-19 (RR 0.30; 95% CI 0.20 - 0.45) (
Table 2).
Multivariate Analysis
We controlled for sex and age as confounding factors. The independent risk factors for contracting COVID-19 were smoking ≥20 cigarettes/day (aRR 8.42; 95% CI 2.02-35.10) and sharing bathrooms and toilets with ≥50 people (aRR 4.28; 95% CI 1.27-14.4). Owning a personal hand sanitiser (aRR 0.20; 95% CI 0.06-0.67) and prior COVID-19 vaccination (aRR 0.16; 95% CI 0.05-0.48) were independent protective factors for contracting COVID-19. Notably sharing a sleeping space with ≥10 people was excluded from the final model, so we failed to reject the null hypothesis: no association between sharing sleeping spaces and contracting COVID-19 (
Table 2).
Measures of Impact
The excess risk for contracting COVID-19 among those who smoked ≥20 cigarettes/day was 34.4 per 100, 40.4% of these can be attributed to this and could be eliminated if they smoked less. The excess risk for contracting COVID-19 in the study population was 10.1 per 100, 19.9% of all COVID-19 cases can be attributed to this factor and could be eliminated if the population smoked less.
The excess risk of contracting COVID-19 among those who shared bathrooms and toilets with ≥50 people was 27.8 per 100, 40.1% of these can be attributed to this and could be eliminated if fewer people shared toilets and bathrooms. In the study population, the excess risk for contracting COVID-19 was 9.1 per 100, 17.9% of COVID-19 cases can be attributed to this factor and could be eliminated if fewer groups of people shared toilets and bathrooms.
Discussion
The objective of our study was to investigate the COVID-19 outbreak among construction workers at Mount Hampden which was reported on 16 February 2021 and to determine workplace risk factors as well as assess epidemic preparedness and response of the district health team. The independent risk factors associated with contracting COVID-19 amongst construction workers at Mount Hampden were smoking >20 cigarettes/day and sharing bathrooms and toilets with more than 50 people whilst owning a hand sanitiser and prior vaccination against COVID-19 were protective factors. Hence the benefit of preventive behaviour and vaccination was shown.
We found that smoking at least a pack of cigarettes/day was an independent risk factor for contracting COVID-19. The significance of smoking in this study population could have been attributed to a high smoking prevalence of 61% in this population. High smoking prevalence has been reported among Asian males, Yang et al., 2016 reported a smoking prevalence of 57.6% [
19]. Social practices like sharing cigarettes are a norm in most Asian communities and have been proven as drivers of transmission [
20],however, in our study this was not an independent risk factor. It is possible that the study population was cautious of sharing cigarettes due to the risk of contracting COVID-19.
Despite our study revealing that there was overcrowding at the construction site, sharing a sleeping space with more than 10 people was not an independent risk factor since it was excluded from the final model. However, sharing bathrooms and toilets was independent risk factor for contracting COVID-19. This could be explained by the overcrowding which we witnessed during the environmental assessment [
18]. Similarly, Rajesh Ludam in 2015 cited that the optimum floor space per individual should range between 4.65 to 9.30 m
2 [
21]. Though workers reported that they maintained minimum physical distancing, workplaces such as construction sites are high-volume sites, where employees commonly work and live in the same place and physical distancing is almost impossible [
22].
We also found that hygiene was poor in the living areas and the barracks had poor ventilation with makeshift window openings. This could have contributed to infection spread, especially in the highly congested barracks C and D. Ramesh et al., 2020 alluded that such workspaces tend to be crowded with commune-type setups, shared toilets, bathrooms and eating spaces [
23]. Like other scholars, he emphasized that in such instances, robustness in worker screening, and defined movement in and out of camps, emphasizing other prevention measures like hand washing and use of facemasks becomes important [
22-24]. This was consistent with our finding that preventive measures were not adequate at this site, with workers easily breaking out of quarantine. This was the probable source of the infection in the first place. The importance of adhering to quarantine and respecting quarantine could have prevented this outbreak. Isolating positive cases was a key action in controlling this outbreak.
Males were twice more likely to contract COVID-19 though this was not an independent risk factor. The construction site is mainly male-dominated and the few females who worked there lived in less crowded barracks. The less congested female living areas could have resulted in a lesser risk of contracting COVID-19. Lorenzo and Trolio in Italy found that males had a higher risk and advancing age was a documented risk factor for COVID-19 [
25]. Similarly, Ng et al in 2021 reported a similar trend in increased risk among males and ages above 35 years [
15]. In other studies, younger age groups have fewer COVID-19 infections and young age is thought to be protective [
26,
27]. Another factor that could have contributed is that younger people have fewer underlying conditions, and in our study, we found that asthma, diabetes mellitus and hypertension were risk factors though not independently associated. The presence of other medical conditions and smoking prevalence with advancing age among males can explain our findings. Earlier COVID-19 outbreak investigations in China also alluded to a combination of these factors being responsible for the high morbidity rates in the older population [
4,
28].
Owning a personal hand sanitiser was independently protective against COVID-19. Those who owned hand sanitisers probably had thorough and consistent hand hygiene. Other protective factors we found were maintaining recommended physical distance and consistent facemasks used during meetings, gatherings or in the workplace. Lyu and Wehby in 2020 also found that consistent and correct use of face masks social distancing and adherence to movement restrictions are protective factors in contracting COVID-19. These measures when fully adhered to can reduce incidence by significant levels [
29,
30].
Prior COVID-19 vaccination was independently protective. COVID-19 vaccines are still fairly new, and we are yet to learn the full extent of their protective effects. However, findings from this study suggest that there is a benefit, of not only getting milder COVID-19 infections but averting incident infections altogether. It has been suggested that vaccination against COVID-19 reduces one´s risk of getting infected, and the risk of getting symptomatic disease, and reduces transmission to other individuals thereby curbing the spread of the pandemic [
31,
32]. These hypotheses could help explain our findings.
The study was not without limitations. Through anticipating language barriers, we used self-administered questionnaires, which may have introduced a response bias. Social desirability bias could have also been present with participants responding to questions in a manner that would make them look good to the researchers.
Conclusion
Smoking more than 20 cigarettes/day and overcrowding resulting in shared bathrooms and toilets were independent risk factors for contracting COVID-19. Almost 20% of infections could have been prevented if the population smoked less and the living area was decongested. Personal hand sanitisers, face mask use and prior COVID-19 vaccination were protective factors. The RRT responded to the outbreak on time.
To prevent workplace outbreaks, regular testing of employees, strict adherence to quarantine rules for visitors and restriction of unnecessary visits were recommended. Meetings were to be held in smaller groups and operate on a rotational roster to allow for physical distancing and easier tracing of contacts during outbreaks. The wardens and supervisors were to ensure reduced movement between staff barracks and staggering break times to ensure adequate spacing in eating spaces and maintenance of a clean living and working environment.
Public Health Actions
With the support of China-AID, all workers at the construction site were fully vaccinated. The government of China, through China-AID collaborated with the Ministry of Health and Child Care, Zimbabwe to have a countrywide outreach program to vaccinate Chinese nationals. This organisation was mandated to protect its citizens in corporate functions, which include mines, industrial sites and construction sites like the Mount Hampden construction site in this study.
What is known about this topic
- The causative agent of COVID-19, signs and symptoms, mode of spread in the community and prevention and control measures.
What this study adds
- The study revealed that there were infection risks in overcrowded construction workplaces worsened by the shared common spaces which has been demonstrated in other settings but not in Zimbabwe.
- The study also provides evidence-based benefits of COVID-19 vaccination.
Competing interests
The authors declare no competing interests.
Authors' contributions
AST: conception, design, analysis, and interpretation of data and drafting of the manuscript. JM: conception, design, analysis, interpretation of data and drafting of the manuscript. EG: conception, design, analysis, interpretation of data and reviewing the draft of the manuscript for intellectual content. TPJ: conception, design, analysis, interpretation of data and reviewing several drafts of the manuscript for intellectual content. NTG: conception, design, analysis, interpretation of data and drafting of the manuscript. MT: conception, design, analysis, interpretation of data and reviewing drafts of the manuscript for intellectual content. The manuscript was read and approved by all authors.
Acknowledgments
We would like to acknowledge the following offices for all the assistance that they rendered, Provincial Medical Directorate Mashonaland West Province, District Medical Officer and Rapid Response Team of Zvimba District and the Health Studies Office, University of Zimbabwe. Many thanks also go to the study participants.
Tables and figures
Table 1: Description of the study population at a Mount Hampden Construction Site
Table 2: Risk factors and independent factors associated with contracting COVID-19
Figure 1: Spot Map - Distribution of COVID-19 cases and attack rates by place of residence at Mount Hampden construction site, constructed from observations during the site visits, 2021
Figure 2: The Epi-curve for the COVID-19 outbreak at Mount Hampden Construction Site, 2021
References
- WHO. Origin of SARS-CoV-2 [Internet]. Geneva (Switzerland): WHO; 2020 Mar 26 [cited 2024 Apr 4]. WHO REFERENCE NUMBER: WHO/2019-nCoV/FAQ/Virus_origin/2020.1.
- Wang C, Horby PW, Hayden FG, Gao GF.A novel coronavirus outbreak of global health concern . The Lancet [Internet]. 2020 Jan 24 [cited 2024 Apr 4];395(10223):470-3. https://doi.org/10.1016/S0140-6736(20)30185-9 Google Scholar
- Lotfi M, Hamblin MR, Rezaei N.COVID-19: Transmission, prevention, and potential therapeutic opportunities . Clinica Chimica Acta [Internet]. 2020 May 29 [cited 2024 Apr 4];508:254-66. https://doi.org/10.1016/j.cca.2020.05.044 PubMed | Google Scholar
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B.Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China . The Lancet [Internet]. 2020 Jan 24 [cited 2024 Apr 4];395(10223):497-506. https://doi.org/10.1016/S0140-6736(20)30183-5 Google Scholar
- Guo YR, Cao QD, Hong ZS, Tan YY, Chen SD, Jin HJ, Tan KS, Wang DY, Yan Y.The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak - an update on the status . Military Med Res [Internet]. 2020 Mar 13 [cited 2024 Apr 4];7(1):11. https://doi.org/10.1186/s40779-020-00240-0 Google Scholar
- WHO. WHO Director-General´s opening remarks at the media briefing on COVID-19 - 11 March 2020 [Internet]. Geneva (Switzerland): WHO; 2020 Mar 11 [cited 2021 Feb 20].
- Chan JFW, Yuan S, Kok KH, To KKW, Chu H, Yang J, Xing F, Liu J, Yip CCY, Poon RWS, Tsoi HW, Lo SKF, Chan KH, Poon VKM, Chan WM, Ip JD, Cai JP, Cheng VCC, Chen H, Hui CKM, Yuen KY.A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster . The Lancet [Internet]. 2020 Jan 24 [cited 2024 Apr 4];395(10223):514-23. https://doi.org/10.1016/S0140-6736(20)30154-9 Google Scholar
- Ministry of Health and Child Care (ZW). Public Health (COVID-19 Prevention, Containment and Treatment) (Amendment) Regulations, 2020 (No. 2): Statutory Instrument 98 of 2020 [Internet]. 2020 May 2 [cited 2024 Apr 4]. Download SI 2020-098 Public Health (COVID-19 Prevention, Containment and Treatment) (Amendment) Regulations, 2020 (No. 2).pdf.
- Ministry of Health and Child Care (ZW). Public Health (COVID-19 Prevention, Containment and Treatment) (National Lockdown) (No. 2) (Amendment): Order, 2021 (No. 13) Statutory Instrument 42 of 2021 [Internet]. Harare (Zimbabwe): Zimbabwean Government Gazette; 2021 Feb 15 [cited 2024 Apr 4]; 2 p. Download SI 2021-042 Public Health (COVID-19 Prevention, Containment and Treatment) (National Lockdown) (No. 2) (Amendment) Order, 2021 (No. 13).pdf.
- Ministry of Health and Child Care (ZW). Public Health (COVID-19 Prevention, Containment and Treatment) (National Lockdown) (No. 2) (Amendment) Order, 2021 (No. 9): Statutory Instrument 10 of 2021. Zimbabwean Government Gazette [Internet]. 2021 Oct 6 [cited 2024 Apr 4]; 5 p. Download zw-government-gazette-dated-2021-10-06-no-118.pdf.
- Dzinamarira T, Mukwenha S, Eghtessadi R, Cuadros DF, Mhlanga G, Musuka G.Coronavirus disease 2019 (COVID-19) response in zimbabwe: a call for urgent scale-up of testing to meet national capacity . Clinical Infectious Diseases [Internet]. 2020 Aug 31[cited 2024 Apr 4];72(10):e667-74. https://doi.org/10.1093/cid/ciaa1301 PubMed | Google Scholar
- UN Office for the Coordination of Humanitarian Affairs. Zimbabwe (DISCONTINUED AS OF 31 DEC 2020) Situation Report. Geneva (Switzerland): UN Office for the Coordination of Humanitarian Affairs; 2021 Feb 19 [last updated 2020 Dec 31; cited 2024 Apr 4]; 20 p. Download Situation Report - Zimbabwe - 31 Dec 2020.pdf.
- Ministry of Health and Child Care (ZW). Zimbabwe Guidelines for the Management of COVID_19 [Internet]. Harare (Zimbabwe): Ministry of Health and Child Care (ZW); 2020 Apr 2 [cited 2024 Apr 4]; 12 p. Download ZIMBABWE_COVID-19-CLINICAL-GUIDELINES-APRIL-2020.pdf
- Herald T. New city takes shape in Mt Hampden.The Herald [Internet]. 2020 Nov 25 [cited 2021 Feb 20]: [about 5 screens].
- Ng OT, Marimuthu K, Koh V, Pang J, Linn KZ, Sun J, De Wang L, Chia WN, Tiu C, Chan M, Ling LM, Vasoo S, Abdad MY, Chia PY, Lee TH, Lin RJ, Sadarangani SP, Chen MIC, Said Z, Kurupatham L, Pung R, Wang LF, Cook AR, Leo YS, Lee VJ.SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: a retrospective cohort study . The Lancet Infectious Diseases [Internet]. 2020 Nov 2 [cited 2024 Apr 4];21(3):333-43. https://doi.org/10.1016/S1473-3099(20)30833-1 PubMed | Google Scholar
- WHO Regional Office for Africa. Technical Guidelines for Integrated Disease Surveillance and Response in the African Region: Third edition [Internet]. Brazzaville (Republic of Congo): WHO Africa; 2019 Mar [cited 2024 Apr 4]: 77 p.
- Hosmer DW, Lemeshow S, Sturdivant RX. Applied logistic regression. Third edition. Hoboken (NJ): Wiley; 2013. 500 p. (Wiley series in probability and statistics). Google Scholar
- UN High Commissioner for Refugees (UNHCR). UNHCR Handbook for Emergencies. Geneva (Switzerland): UN High Commissioner for Refugees (UNHCR); 2007 Feb [cited 2024 Apr 4]; 595 p. Download Handbook for Emergencies. Google Scholar
- Yang T, Barnett R, Jiang S, Yu L, Xian H, Ying J, Zheng W. Gender balance and its impact on male and female smoking rates in Chinese cities . Social Science & Medicine [Internet]. 2016 Feb 24 [cited 2024 Apr 4];154:9-17. https://doi.org/10.1016/j.socscimed.2016.02.035 PubMed | Google Scholar
- Gautret P, Colson P, Lagier JC, Parola P, Raoult D.Does spitting in public play a role in transmitting SARS-CoV-2? Travel Medicine and Infectious Disease [Internet]. 2020 May 31 [cited 2024 Apr 4];36:101759. https://doi.org/10.1016/j.tmaid.20101759 PubMed | Google Scholar
- Rajesh Ludam. Housing & Ventilation [slides]. San Francisco (CA): Slideshare; 2015 Sep 7 [cited 2024 Apr 5]. 29 slides. Google Scholar
- Wong ELY, Ho KF, Wong SYS, Cheung AWL, Yau PSY, Dong D, Yeoh EK. Views on workplace policies and its impact on health-related quality of life during coronavirus disease (COVID-19) pandemic: cross-sectional survey of employees . Int J Health Policy Manag [Internet]. 2020 Aug 3 [cited 2024 Apr 4];13(3): 344-53. https://doi.org/10.34172/ijhpm.2020.127 PubMed | Google Scholar
- Ramesh N, Siddaiah A, Joseph B.Tackling corona virus disease 2019 (COVID 19) in workplaces . Indian J Occup Environ Med [Internet]. 2020 Mar 18 [cited 2024 Apr 4];24(1):16-18. https://doi.org/10.4103/ijoem.IJOEM_49_20 PubMed | Google Scholar
- HM Government. Working safely during COVID-19 in construction and other outdoor work: COVID-19 secure guidance for employers, employees and the self-employed [Internet]. London (United Kingdom): UK Health Security Agency; 2020 May 11[last updated 2020 Nov 5; cited 2024 April 4]. 41 p. Google Scholar
- Di Lorenzo G, Di Trolio R.Coronavirus disease (COVID-19) in Italy: analysis of risk factors and proposed remedial measures. Front Med [Internet]. 2020 Apr 9 [cited 2024 Apr 4];7:140. https://doi.org/10.3389/fmed.2020.00140 Erratum in: Corrigendum: Interferon-∝2b Treatment for COVID-19 . Front Immunol [Internet]. 2020 Oct 27 [cited 2024 Apr 4];11:615275. https://doi.org/10.3389/fimmu.2020.615275 PubMed | Google Scholar
- CDC COVID-19 Response Team.Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019 - United States, February 12-March 28, 2020 . MMWR Morb Mortal Wkly Rep [Internet]. 2020 Apr 3 [cited 2024 Apr 4]; 69(13);382-386. http://dx.doi.org/10.15585/mmwr.mm6913e2 PubMed | Google Scholar
- Klang E, Kassim G, Soffer S, Freeman R, Levin MA, Reich DL.Severe obesity as an independent risk factor for covid–19 mortality in hospitalized patients younger than 50 . Obesity [Internet]. 2020 May 23 [cited 2024 Apr 4];28(9):1595-9. https://doi.org/10.1002/oby.22913 PubMed | Google Scholar
- Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, Huang H, Zhang L, Zhou X, Du C, Zhang Y, Song J, Wang S, Chao Y, Yang Z, Xu J, Zhou X, Chen D, Xiong W, Xu L, Zhou F, Jiang J, Bai C, Zheng J, Song Y.Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in wuhan, china . JAMA Intern Med [Internet]. 2020 Mar 13 [cited 2024 Apr 4];180(7):934-43. https://doi.org/10.1001/jamainternmed.2020.0994 PubMed | Google Scholar
- Zhang Y, Jiang B, Yuan J, Tao Y.The impact of social distancing and epicenter lockdown on the COVID-19 epidemic in mainland China: A data-driven SEIQR model study . medRxiv 2020.03.04.20031187 [Preprint]. 2020 [posted 2020 Mar 6; cited 2024 Apr 4]: [11 p.]. https://doi.org/10.1101/2020.03.04.20031187 Google Scholar
- Lyu W, Wehby GL.Community use of face masks and covid-19: evidence from a natural experiment of state mandates in the us: study examines impact on covid-19 growth rates associated with state government mandates requiring face mask use in public . Health Affairs [Internet]. 2020 Jun 16 [cited 2024 Apr 4];39(8):1419-25. https://doi.org/10.1377/hlthaff.2020.00818 PubMed | Google Scholar
- CDC. Benefits of Getting a COVID-19 Vaccine [Internet]. Geneva (Switzerland): CDC; 2023 Sep 22 [cited 2021 Jun 20]. [about 5 screens]. Google Scholar
- Hodgson SH, Mansatta K, Mallett G, Harris V, Emary KRW, Pollard AJ.What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2 . The Lancet Infectious Diseases [Internet]. 2020 Oct 27 [cited 2024 Apr 4];21(2):e26-35. https://doi.org/10.1016/S1473-3099(20)30773-8 PubMed | Google Scholar