Descriptive Epidemiology of Measles Cases in Zamfara State—Nigeria, 2012-2018
Fatima Muhammad Garba1,&, Rabi Usman2, Chukwuma Umeokonkwo1,3, Emmanuel Chukwudi Okolocha4, Mohammed Yahaya1,5, Ibrahim AbdulQadir6, Okunromade Oyeladun7, Augustine Olajide Dada8, Muhammad Shakir Balogun1
1Nigeria Field Epidemiology and Laboratory Training Programme, Abuja, Nigeria, 2Zamfara State Ministry of Health, Gusau, Zamfara State, Nigeria, 3Department of Community Medicine, Federal Teaching Hospital, Abakaliki, Ebonyi State, Nigeria, 4Department of Veterinary Public Health, Ahmadu Bello University, Zaria, Kaduna State, Nigeria, 5Department of Medical Microbiology and Parasitology, Usmanu Danfodiyo University, Sokoto, Sokoto State, Nigeria, 6Department of Hematology and Blood Transfusion, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Sokoto State, Nigeria, 7Nigeria Centre for Disease Control, Abuja, Nigeria, 8Africa Field Epidemiology Network, Abuja, Nigeria
&Corresponding author
Fatima Muhammad Garba, Nigeria Field Epidemiology and Laboratory Training Network, African Field Epidemiology Network, 50 Hallie Selassie Street, Asokoro, 900231, Abuja, Nigeria. fatimagarba19@gmail.com
Introduction:
Nigeria still experiences recurrent outbreaks of measles especially in the North despite the efforts at strengthening routine immunisation and supplementary immunisation activities. We analysed measles surveillance data from Zamfara State, northwestern Nigeria to identify variations in distribution across ages, gender, place, trends, and seasonality.
Methods:
We conducted a secondary data analysis of measles surveillance data collected between 2012 and 2018 from all the local government areas (LGA) in Zamfara State, obtained from Zamfara State Ministry of Health in an electronic line list. We calculated frequencies and proportions for descriptive statistics and used time series analysis to determine the trend and seasonality.
Results:
A total of 1,023 measles cases were recorded between January 2012 and December 2018. The median age was 2.3 years (range: 6 months-37 years). The males recorded a slightly higher proportion of cases (50.5%). As age increases the incidence was found to decrease, with the highest attack rate (120.8/100,000 population) among the under-five age group. The urban areas had the highest attack rate with the state capital (Gusau LGA) having the highest attack rate. Similar trend of measles cases was observed over the years of study and computed seasonal variation revealed the highest incidence in the first quarter. Overall case fatality rate (CFR) over the years was 4.8%.
Conclusion:
The study recorded a high burden of measles in under five age group and in urban areas with potential interaction of insecurity on the measles control and elimination program. Therefore, the existing framework on measles control strategies for successful elimination of the disease should be strengthened among the under-five age group and urban areas.
Introduction

Measles is an infectious febrile rash illness caused by the measles virus that affects mostly children under the age of five years. It was implicated in millions of deaths before the advent of the measles vaccine [1-3]. Despite the availability of a safe and effective vaccine, globally measles is one of the leading vaccine-preventable diseases that cause disability and death in childhood, especially among the under five years [1,4]. In 2016 globally, an estimated seven million people were affected by measles while mortality from measles has declined by 84 percent; from 550,100 deaths in 2000 to 89,780 [1]
In 2018, the African region reported a total of 56,146 suspected cases of measles, out of which 24,847 were confirmed as measles. During the same period in 2018, Nigeria recorded about 6,593 confirmed cases of measles and a 12- month rolling measles incidence rate of 36.3 per 1,000,000 total population [
5].
Nigeria has the largest population in Africa with over 180 million people and measles is the fifth leading cause of under-five child mortality in Nigeria [
6,
7]. Measles transmission occurs all year round in Nigeria with increased incidence in the dry season due to the occurrence of outbreaks [
4]. The 2018 National Demographic and Health Survey (NDHS) data indicated that about 31% of children 12-23 months of age had received vaccines appropriate for their age. Nationally, measles vaccination coverage was 54% while Zamfara State recorded 12.2% [
8]. The southern part of the country had higher measles vaccination coverage than the northern part as indicated by the 2016-2017 Nigeria Multiple Indicator Cluster Survey (MICS) and National Immunization Coverage Survey (NICS): South-East - 72.6%, South-West - 71.7%, South-South - 69.0%, North-Central- 52.4%, North-East -36.0%, and North-West - 22.4% respectively. Zamfara State is among the seven states in the North-West geopolitical zone of Nigeria and had measles vaccination coverage of 16.2% among the 12-23 months age group [
9].
Due to the high prevalence of measles in Africa, the African Region of the World Health Organization (WHO) developed a strategic plan as part of the measles elimination goal which was adopted by Nigeria; to be achieved by 2020. The strategies are: strengthening routine immunization with a two dose-schedule with the measles-containing vaccine (MCV) to increase protection in children; the first dose of the vaccine at 9 months of age and the second dose in the second year of life. Conducting recurrent measles vaccination campaigns through SIAs; at intervals of two years. Implementation of case-based measles surveillance to enable prompt monitoring and adjustment of immunization strategies, supported by the measles laboratory network. And the provision of standard case management for measles cases in accordance with the Integrated Management of Childhood Illnesses (IMCI) protocols.
Despite the efforts at strengthening Routine Immunisation (RI) and Supplementary Immunisation Activities (SIA), recurrent outbreaks of measles still occur in Zamfara State. Thus, the need to evaluate the measles surveillance data which is crucial in informing and guiding policy making, control strategies, and improvement in data collection for successful elimination of the disease in Nigeria. Therefore, we evaluated the measles surveillance data from 2012 to 2018 to identify variations in distribution across ages, gender, place, trends, and seasonality.
Methods

Study setting
Zamfara State, northwestern Nigeria had a projected total population of 4,757,222 in 2018 (based on the 2006 Census population with an annual growth rate of 3.2%). Zamfara has a tropical climate with a temperature rising to 38°C (100.4°F) and above between March and May. The rainy season usually occurs between March and November while the dry season is between October and June [
4]. The state has a total of 712 health facilities distributed across 14 LGAs. These health facilities include; 71 Primary Health Centers (PHC), 607 Health Clinics, 10 private hospitals, 22 General Hospitals, 1 Specialist Hospital, and 1 Federal Medical Center [
10]. Secondary and Tertiary health facilities and urban PHCs offer daily RI fixed sessions while the rural PHCs conduct at least one fixed session and one outreach session per week through the Optimised Integrated RI Sessions (OIRIS) coordinated by National Emergency Routine Immunisation Coordination Center (NERICC) [
11]. The majority of the PHCs and health clinics offer treatment services for uncomplicated measles cases while the complicated cases are referred to secondary and tertiary health facilities.
Study design
We conducted a retrospective secondary data analysis of measles surveillance data from the Integrated Disease Surveillance and Response (IDSR) records in Zamfara State between January 2012 and December 2018 using a quantitative method.
Measles surveillance
The measles surveillance system is a passive, case-based system operated by Disease Surveillance Notification Officers (DSNOs), doctors, laboratorians, nurses, community health extension workers, and environmental health officers. Measles cases were reported on weekly bases on the IDSR system using the IDSR 002 reporting form and 001A (case investigation form) [
2]. Information is channeled from the health facilities, through the ward focal persons to the Local Government DSNOs, to the State DSNO, to the State Epidemiologist, and then to the Federal Ministry of Health. Feedback is provided in the opposite direction. A suspected case of Measles is defined as any person with fever and maculopapular (non-vesicular) generalised rash and cough, coryza or conjunctivitis, or any person in whom a clinician suspects Measles. A confirmed case is a suspected case with laboratory confirmation (positive IgM antibody) or epidemiological link to confirmed cases in an outbreak. If the number of confirmed measles cases exceeds three in any catchment area or health facility in one month, an outbreak is declared and all suspected cases are then line-listed at the health facility level and data is shared with LGA, State, and National [
12].
Data source
Integrated Disease Surveillance and Response (IDSR) weekly epidemiological data between January 2012 and December 2018 were obtained from the Epidemiology Unit of Zamfara State Ministry of Health in an electronic format. Population estimates were made from the National Population Commission 2006 census figures, using the 3.2% annual growth rate for Zamfara State.
Data management
Data abstraction and study variables
The IDSR weekly epidemiological measles data throughout the study were extracted from an electronic line list, in Microsoft Excel file format. The variables included on the spreadsheet were age, sex, date of onset of symptoms, and outcome (dead/alive). The electronic database consisted of 1,129 records. However, in our analysis, we only included those records with complete data on at least three variables. With this, we excluded 106 (9%) records. Data cleaning was done to check for completeness and accuracy of data, efforts were made to ascertain the true status of missing data before declaring them as such.
Statistical analyses
Data were recorded and analysed using Microsoft Excel 2016 and mapping was done using Quantum Geographic Information System (QGIS). A descriptive analysis was carried out to characterise the measles cases in person, place, and time. The Attack Rate and CFR were calculated using the measles cases/deaths per the specific population at risk. The trend of measles cases over the seven years was examined using time series analysis. The data were aggregated in quarters (3-months) as 1st quarter (January - March), 2nd quarter (April-June), 3rd quarter (July-September), and 4th quarter (October-December) to represent the 4-quarters in a year from 2012 to 2018 which was computed into a 3-monthly moving average to adjust for the seasonal variations (SV) from the data. To obtain the number of cases in a quarter and the trend line, we applied the seasonal variation method using the multiplicative model based on the observed pattern in the data mathematically represented as follows [
13];

Where; Yt represented the number of cases in a quarter
Tt represented the trend line derived from the mathematical equation;
The data was deseasonalised to obtain the variation in each quarter of the year using the adjustment factor (AF) derived from the equation[
13];

Therefore, Quarterly variation (
QVi) =

Table 1 and
Table 2 shows the procedures involved in the estimation of quarterly variation and deseasonalisation of seasonal variation.
Figure 1 shows the monthly pattern merged into a quarter on yearly basis and smoothed using a time series approach to obtain the trend.
Ethical consideration
We obtained administrative approval from the Public Health Department of Zamfara State Ministry of Health before collecting the measles IDSR case-specific data set. Ethical approval was also obtained from the ethical committee of the State Ministry of Health. For confidentiality, personal information was concealed by excluding identifiable information like name and address. Data was protected by ensuring that only the research team had access to the dataset during extraction and analysis.
Results
A total of 1,023 measles cases were recorded in Zamfara State between January 2012 and December 2018 across all 14 LGAs. The median age was 2.3 years with (range: 6 months to 37 years). The highest number of cases - 841 (82.2%) - were recorded in those less than 5 years old and the least was in those 15 years and above - 7 (0.7%) Table 3. The males recorded a slightly higher proportion of cases (50.5%) than females. Further analysis of cases in the under-five age group revealed the highest proportion of cases (32.70%) in the age-group one to two years and the least (7.73%) in those younger than one year of age. The overall eight-year CFR is 4.8%. Age-specific Attack Rate (AR) declined as age increased with the highest in under-five children (120.8/100,000) but the age-specific CFR was highest (6.3%) in those aged 5-9 years Table 4.
Most cases (36.3%) and deaths (2.2%) were recorded in Gusau LGA, no death was recorded in Bukkuyum, Kaura-Namoda, Maradun, and Tsafe LGAs. The highest AR (96.8/100,000 population) was also recorded in the Gusau LGA (the state capital) and the least (3.8/100,000) was in Maradun LGA
Figure 2.
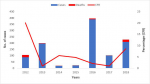
The majority of cases, 389 (38.0%), were reported in 2016 and the least was in 2014(5.6%) which also applies to the yearly incidence of measles with the highest in 2016 (8.7/100,000 population) and the lowest in 2014 (0.4/100,000 population). The CFR per year was highest in 2012 (20.1%)
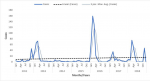
Figure 3. The trend of the cases showed a similar pattern throughout the years under review with a slight positive correlation of 0.079
Figure 4. The first quarter had the highest seasonal variation which was across all the years of study and the lowest in the third quarter as shown in
Figure 1.
Discussion
The 2012 to 2018 measles surveillance data description in Zamfara State reveals the highest number of cases in the under-five years' age group, however, the age-specific CFR was more in those aged five to nine years. More cases occurred in the urban areas especially in the state capital (Gusau LGA) and the trend of occurrence of the disease was highest in the first quarter of the year throughout the years of study.
The greater burden observed in the under-five years´ age group is a similar finding in some studies conducted in Nigeria and some developing countries [
14,
15]. This is unexpected considering the measles control measures established within the country through the availability of free and effective measles vaccines administered during routine immunisation and SIA targeted at the under-five age group. The lower incidence among the age groups of five years and above could be due to lifelong immunity acquired through measles infection and/or possible exposure to the antigen through vaccination. Our study also identified that among the under-five group, children aged between one and two years recorded the highest number of cases which could be due to the low vaccination coverage of 16.2% among this age group in Zamfara State [
16]. A study showed that determinants of the average age of acquiring measles are mainly population immunity and birth rate; low population immunity, high birth rates, and high population density lead to increased transmission in younger age groups commonly seen in developing countries [
17]. An increase in vaccination coverage can influence the average age of acquiring measles infection; from the younger age group to adolescents and young adults [
17].
The seven-year CFR of 4.8% is in range with the CFR reported from other studies in Nigeria with a range of 3-5% which could be as high as 10% for developing countries [
1,
14]. Despite the decrease in the incidence of measles as age increases, age-specific CFR was found to be highest in 5-9 years of age. This finding is contrary to other related studies conducted in Nigeria where the under-five age group showed a higher mortality rate [
7,
15].
The slight male preponderance in the cases is not a significant finding because the lack of categorical sex-specific population data per age group for estimation of sex-specific attack rate hinders the determination of the disease burden per sex. However, some studies also revealed a slight male preponderance [
15,
18]. A study revealed that females become infected earlier than males because they may lose maternal antibodies earlier than boys [
19].
The state capital; Gusau LGA harbors a significant burden possibly due to increased population density from the outmigration of pastoralists and other community members from areas most affected by cattle rustling and armed banditry. It was revealed by a study that as much as 80% to 90% of the pastoralists migrate to the State Capital or other States [
20]. Local Government Areas with the lowest attack rate like Zurmi, Shinkafi, Tsafe, and Kaura-Namoda were among the worst affected by insecurity, therefore, leading to outmigration of the communities. Zamfara State had always recorded poor health indices including poor immunisation coverage in the country [
8,
16]. A study on Routine Immunisation (RI) coverage survey recorded poor coverage in the following LGAs; Gusau (10%), Bungudu (11%), Bukkuyum (14%), Maradun (20%), and Shinkafi (25%) [
21]. Therefore, the high population density and poor RI coverage in Gusau LGA explain the high attack rate in the urban part of the State. A similar finding in a study highlighted the occurrence of lesser measles cases in rural than in urban settings [
18].
The lowest number of cases recorded in 2014 could be explained by the information from the State Ministry of Health which revealed that there were no active surveillance officers during the period and new surveillance officers were recruited in 2016, hence the resurgence in 2016. Despite the SIA in 2015 and 2017, large outbreaks occurred in 2016 and 2018 possibly due to the poor RI coverage and immunisation campaigns which may not have reached the targeted populations, especially in the security-compromised area. The drastic decline of the CFR in the year 2013 could be from intensified surveillance, and effective case management due to the high fatality in 2012 and SIA carried out in 2012/2013.
The seasonal pattern in this study exhibited an increased incidence of measles during the dry season (October to May) which peaks in the first quarter. A similar finding was also reported from previous studies on measles epidemiology within the country and WHO African region [
14,
4]. These findings from our study signify that the cornerstone in measles control is the strengthening of RI coverage and SIAs reaching every ward. Studies have shown that one dose of measles vaccination confers about 85% seroconversion when given at 9 months and seroconversion after second-dose measles vaccination is >99% when the second dose is given at
≤12 months [
1]. Hence, the need to strengthen the newly implemented administration of the second dose of the measles-containing vaccine (MCV2) in Nigeria.
The study experienced some limitations; mainly incompleteness of data (this led to exclusion of 9% of the data during analysis) of which 88% of cases had missing entries on vaccination status. It also had some missing variables such as laboratory findings and hospitalization status. The surveillance data was generated from reported cases so the surveillance system may not have captured all cases in the State during the study period which could lead to an underestimation of the number of measles cases. Despite the limitations, we described the measles epidemiology over seven years and we hope to conduct analytical studies that would further evaluate the disease.
Conclusion
Over the years of study, measles remains a great burden among the under-five years’ age group and urban areas of Zamfara State. Also, measles infection and mortality occurred throughout the reviewed years with a peak in cases in the first quarter of the year. Therefore, we recommend more emphasis on strengthening the existing framework on measles control strategies by giving more attention to measles surveillance, routine immunisation, and supplementary immunisation activities to reach every ward and under-five age group. There is also a need for refresher training of frontline surveillance officers on the appropriate filling of measles reporting tools for successful eradication of the disease.
What is known about this topic
- The study retrospectively described seven-year measles surveillance data and it has been previously known that the burden of measles is highest among the under-five age group
- Additionally, the seasonal pattern of measles occurrence has been highest in the dry season (Oct. to May) where the first quarter of the year falls as highlighted by our study.
What this study adds
- This study revealed more information on the seven-year trend of measles cases in Zamfara State, north-western Nigeria highlighting the potential interaction of insecurity with measles control measures
- The study also utilised routine surveillance data to estimate trends and rates which is crucial in informing and guiding policy making, control strategies, and improvement in data collection for successful eradication of the disease in Nigeria.
Competing interests
The authors declare no competing interests.
Authors' contributions
FMG led the designing of the study, the acquisition of an electronic dataset from the Zamfara State Ministry of Health, and subsequent analysis. FMG wrote the drafts of the manuscript and revised the paper for substantial intellectual content. RA, CU, ECO, MY, IA, OO, DA, and MSB participated in the design, and analysis of the study and reviewed the draft manuscript, providing substantial intellectual involvement. All authors reviewed, read, and approved the final manuscript.
Acknowledgments
We gratefully acknowledge the support of Zamfara State Ministry of Health and Africa Field Epidemiology Network Abuja, who provided expertise that greatly assisted in the study. We thank the following Residents of the Nigeria Field Epidemiology and Laboratory Training Program (Aisha Sani Farouq, Ahmad Njidda, Azuka Adeke) for providing study materials essential for the study.
Tables and figures
Table 1: seasonal variation of measles cases in Zamfara State—Nigeria, 2012-2018
Table 2: deseasonalisation of seasonal variation of measles cases and estimation of the quarterly variation in Zamfara State—Nigeria, 2012 to 2018
Table 3: distribution of Measles Cases by Age, Sex, and Outcome in Zamfara State—Nigeria, 2012-2018
Table 4: age-specific attack rate per 100,000 population and case fatality rate [CFR] of measles, Zamfara State—Nigeria, 2012-2018
Figure 1: frequency distribution of quarterly reported cases (Yt) of measles and the trend line (Tt), Zamfara State—Nigeria, 2012-2018
Figure 2: map of Zamfara State showing measles attack rate by LGA, 2012 to 2018
Figure 3: distribution of measles cases, death and case fatality rate (CFR) in Zamfara State—Nigeria, 2012-2018
Figure 4: trend of Measles Cases by Months in Zamfara State—Nigeria, 2012-2018
References
- WHO. Measles. WHO. 2018[cited 2022 Nov 15].
- Ameh CA, Sufiyan MB, Jacob M, Waziri NE, Olayinka AT. Evaluation of the Measles Surveillance System in Kaduna State, Nigeria (2010-2012). Online J Public Health Inform. 2016 Nov [cited 2022 Nov 15]28;8(3):e206.https://doi.org/10.5210/ojphi.v8i3.7089 PubMed | Google Scholar
- Dayan GH, McLean HQ. Measles. In: International Encyclopedia of Public Health. Elsevier. 2017[cited 2022 Nov 15].
- Ibrahim BS, Usman R, Mohammed Y, Datti Z, Okunromade O, Abubakar AA, Nguku PM. Burden of measles in Nigeria: a five-year review of casebased surveillance data, 2012-2016. Pan Afr Med J. 2019 Jan 22[cited 2022 Nov 15]; 32(Suppl 1):5.https://doi.org/10.11604/pamj.supp.2019.32.1.13564 PubMed | Google Scholar
- WHO. Measles and Rubella Surveillance Data. WHO. 2019[cited 2019 Mar ].
- National Bureau of Statistics, Nigeria. Population - OpenData for The National Bureau of Statistics, Nigeria. Nigeria, National Bureau of Statistics. [cited 2019 Mar ].
- Onoja AB, Adeniji AJ, Faneye A. Measles complications in a Nigerian hospital setting. Clin Rev Opin. 2013; 5(2):18-23. Google Scholar
- National Population Commission, Nigeria. The Federal Republic of Nigeria Nigeria Demographic and Health Survey 2018 National Population Commission Abuja, Nigeria Nigeria, National Population Commission. 2019[cited 2020 Oct ].
- Nigerian Bureau of Statistics, Nigeria. Nigeria - Multiple Indicator Cluster Survey/National Immunization Coverage Survey 2016-17, Fifth round (MICS) and NICS (third Round) - Overview. Nigeria, Nigerian Bureau of Statistics. 2016[cited 2022 Nov 15].
- Usman R, Umar AA, Gidado S, Gobir AA, Obi IF, Ajayi I, Ajumobi O. Predictors of malaria Rapid Diagnostic Tests' utilisation among healthcare workers in Zamfara State. PLoS One. 2018 Dec 14[cited 2022 Nov 15]; 13(12):e0200856.https://doi.org/10.1371/journal.pone.0200856 PubMed | Google Scholar
- WHO. NERICC-Nigeria´s panacea to routine immunization and primary health care strengthening. WHO Regional Office for Africa.2019 [cited 2022 Nov 15].
- WHO & CDC. IDSR Technical Guidelines in the African Region, 2nd Edition. WHO Afro. 2010[cited 2022 Nov 15].
- Cryer, D J, Chan, Kun-sik. Time Series Analysis: With Applications in R[Internet]. New York, NY: Springer; 2008 [cited 2022 Nov 15]. (Casella G, Fienberg S, Okin I, editors. Springer Texts in Statistics).
- Saleh JE. Trends of measles in Nigeria: A systematic review. Sahel Medical Journal. 2016 Jan 1[cited 2022 Nov 15]; 19(1):5-11. https://doi.org/10.4103/1118-8561.181887 Google Scholar
- Faruk AS, Adebowale AS, Balogun MS, Taiwo L, Adeoye O, Mamuda S, Waziri NE. Temporal trend of measles cases and impact of vaccination on mortality in Jigawa State, Nigeria, 2013-2017: a secondary data analysis. Pan Afr Med J. 2020 Feb 19[cited 2022 Nov 15]; 35(Suppl 1):13.https://doi.org/10.11604/pamj.supp.2020.35.1.19780 PubMed | Google Scholar
- National Bureau of Statistics, Nigeria. Nigeria - Multiple Indicator Cluster Survey 2016-2017. Nigeria, National Bureau of Statistics. [cited 2022 Nov 15].
- World Health Organization, editor. Measles vaccines: WHO position paper – April 2017. Weekly Epidemiological Record [Internet]. 2017 Apr 28 [cited 2022 Nov 15];92(17):205–28 English, French, Spanish, Russian.
- Goodson JL, Masresha BG, Wannemuehler K, Uzicanin A, Cochi S. Changing Epidemiology of Measles in Africa. J Infect Dis. 2011 Jul 1[cited 2022 Nov 15]; 204(Supplement 1):S205-14.https://doi.org/10.1093/infdis/jir129 . Google Scholar
- Aaby P, Schenck-Gustafsson K, DeCola PR, Pfaff DW, Pisetsky DS (eds): Handbook of Clinical Gender Medicine. Basel: Karger; 2012[cited 2022 Nov 15] . p 405-413.https://doi.org/10.1159/000336439 . Google Scholar
- Olaniyan A, Yahaya A. Cows, Bandits, and Violent Conflicts: Understanding Cattle Rustling in Northern Nigeria. Africa Spectr. 2016 Dec 1[cited 2022 Nov 15]; 51(3):93-105.https://doi.org/10.1177/000203971605100305 . Google Scholar
- Gunnala R, Ogbuanu IU, Adegoke OJ, Scobie HM, Uba BV, Wannemuehler KA, Ruiz A, Elmousaad H, Ohuabunwo CJ, Mustafa M, Nguku P, Waziri NE, Vertefeuille JF. Routine Vaccination Coverage in Northern Nigeria: Results from 40 District-Level Cluster Surveys, 2014-2015. PLoS One. 2016 Dec 9[cited 2022 Nov 15]; 11(12):e0167835. https://doi.org/10.1371/journal.pone.0167835 PubMed | Google Scholar