Trend of Visceral Leishmaniasis at Medicine Sans Frontier's Abdurafi Treatment Center, West Armachiho District, Ethiopia, 2009-2015, a retrospective descriptive analysis
Sisay Awoke1,&, Sefonias Getachew2, Yimer Seid2, Tatek Bogale3
1Amhara Public Health Institute, Bahir Dar, Ethiopia, 2School of Public Health College of Health Science, Addis Ababa University, Ethiopia, 3Ministry of Health, Addis Ababa, Ethiopia
&Corresponding author
Sisay Awoke, Amhara Public Health Institute, Bahir Dar, Ethiopia. sisaya16@gmail.com
Introduction:
Leishmaniasis currently threatens 350 million men, women and children around the world. Visceral leishmaniasis (VL) is a fatal parasitic disease mostly prevalent in low land areas VL typically affects migrant agricultural workers. Visceral leishmaniasis is caused by the Leishmaniasis donovani complex, which includes Leishmaniasis donovani and Leishmaniasis infantum. An estimated 200,000 to 400,000 new cases of visceral leishmaniasis occur worldwide each year. This study aims to understand the trend, magnitude and mortality of visceral leishmaniasis at MSF Abdurafi treatment center during the period (2009-2015).
Methods:
Retrospective secondary data analysis was conducted on monthly kala-azar report of MSF Abderafi treatment center in West Armachiho district. We included a total of 11680 patients screened for leishmaniasis in 2009-2015. We entered and analyzed data using Microsoft Excel.
Results:
Among 11680 patients screened for kalazar in the study period (2009-2015), 2131 were primary kalazar cases, 198 kalazar were relapse and 19 were post kalazar dermal leishmaniasis. The case fatality of kalazar ranged from 0.9% (4/469) in 2014 to 7.4% (22/296) in 2013. The highest cure rate was (96%) in 2015, and the least was (89%) in 2009. The total case fatality rate during study period was 4% (92/2263). The highest HIV/Kala-azar coinfection rate was 15% in 2009 and the lowest was 4.8% in 2014.
Conclusion:
Visceral leishmaniasis was highly prevalent in the study area. There was high kala-azar mortality rate and majority of deaths were unrecognized. Prevalence rate of VL-HIV co-infection and relapse was higher at MSF Abdurafi kalazar treatment center in West Armachiho district. Ministry of health should strengthen prevention and control mechanisms of kala-azar. Ministry of health and MSF Holland should conduct further studies on the cause of death among kala-azar patients, because there may be drug toxicity or other complications.
Introduction

Visceral leishmaniasis (VL), also known as kala-azar from a Hindi term meaning "black fever" is caused by the L. donovani complex, which includes L. donovani and L. infantum (the latter designated L. chagasi in the New World); these species are responsible for anthroponotic and zoonotic transmission, respectively. India, Nepal, Bangladesh, Sudan, and Brazil are the four largest foci of VL and account for 90% of the world's VL burden, with India being the worst affected. Zoonotic VL has been reported in all countries in the Middle East, Pakistan, and other countries from western Asia to China. Endemic foci also exist in the independent states of the former Soviet Union, mainly Georgia and Azerbaijan. In the Horn of Africa, Sudan, Ethiopia, Kenya, Uganda, and Somalia report VL. In Sudan, large outbreaks are thought to be anthroponotic, although zoonotic transmission also occurs. VL is rare in West and sub-Saharan Africa.
Leishmaniasis occurs in 98 countries, most of which are developing countries in tropical and temperate regions. Two million cases occur annually, of which 1-1.5 million are CL (and its variations) and 500,000 are VL. More than 350 million people are at risk, with an overall prevalence of 12 million. Although the distribution of Leishmaniasis is limited by the distribution of sand fly vectors, human leishmaniasis is on the increase worldwide [
1].
A concomitant HIV infection increases the risk of developing active VL by between 100 and 2320 times. In southern Europe, up to 70% of cases of visceral leishmaniasis in adults are associated with HIV infection [
2].
The risk of treatment failure for VL is high, regardless of the drug used, and all co-infected patients will relapse - and eventually die - unless they are given antiretroviral therapy (ART) [
3].
The visceral form is present in 70 countries. The largest focus of VL is in the south-east Asian region, with an estimated 300 000 cases in 2006. East Africa has approximately 30 000 cases per year [
4].
The reported case fatality rate for VL in Brazil was 7.2% in 2006. In the Indian subcontinent, the focus responsible for the largest proportion of global VL cases, reported case fatality rates ranging from 1.5% (93 deaths/6224 VL cases from 2004-2008) in Bangladesh to 2.4% (853/34,918) in India and 6.2% (91/1477) in Nepal [
5].
Methods

Retrospective secondary data analysis was conducted at MSF Abderafi treatment center. We included a total of 11680 patients screened for leishmaniasis from 2009-2015, and data was retrieved based on screening status. Data was entered and analyzed using Microsoft Excel. The case definition of visceral leishmaniasis (VL) is a person who presents with fever for more than two weeks and an enlarged spleen (splenomegaly) and/or enlarged lymph nodes (lymphadenopathy), or either loss of weight, anemia or leucopenia while living in a known VL endemic area or having travelled to an endemic area and confirmed by laboratory. The commonly available serological tests in the treatment center were RK39 rapid diagnostic test (RDT) and the direct agglutination test (DAT). A support letter written by Amhara Public Health Institute for the district was used to collect and analyze the aggregated data to ensure compliance with ethical considerations.
Results
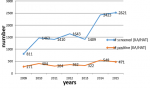
There was a total of 11680 people screened for Kalazar with in the period of 2009 to 2015. From these 1180 screened, 2682 were positive for kalazar making which was 23 % of total positivity rate Figure 1 Of the total screened kalazar patients, the highest positivity rate was 33% in 2009, and the lowest was 19% in 2015. Out of 2682 kalazar (positive) patients, 2343 (87%) commenced treatment. Of a total number of patients who commenced treatment, 2131 cases were primary kalazar, 198 cases were relapse, and 19 cases were post kalazar dermal leishmaniasis Figure 2. Of the patients who commenced treatment during 2009 to 2015, 2096 (92.6%) were cured, 2263 were exited/disqualified (from) the treatment, 92 (4%) died, and 18 (0.18) patients were defaulted.
From 2009 to 2015, there was a total of 198 relapse. The highest relapse cases were 41 in 2011 and the lowest were 15 in 2009, Kala-azar positivity rate, cure rate and relapsing rate.
In the period of 2009-2015 kalazar positivity rate was decreased. There was high positivity rate of 33% in 2009.
Among the 2263 exited kalazar patients from treatment, 2096 (92%) were cured. The lowest cure rate was 89% in 2009 and the highest was 96% in 2015. In the study period, the least and the highest kala-azar relapse rate was 6% and 16% in 2009 and 2011 respectively as shown in
Figure 3.
Mortality rate
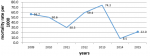
In the period of 7 years (2009-2015), 92 kalazar patients died with mortality rate of 40.6 per 1000 population. In 2013 kalazar mortality rate was 74.3 per 1000 population which was highest as compared with the rest of 7 years´ mortality rate. In 2014 kalazar mortality rate was 8.5 per 1000 population, which was the lowest as compared with the rest of 7 years´ mortality rate of kalazar,
Figure 4.
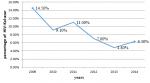
The trend of HIV- Kala-azar co-infection rate in seven years was decreasing in regular manner except in 2011,
Figure 5.
In this study, on average 13 persons (92/2263) per year died of visceral leishmaniasis during the study period. The VL fatality rate reported by MSF Holland at Abdurafi kalazar treatment center was 4% (92/2263) cases from 2009-2015, which was lower than hospital-based of 7.2% in Brazil in 2006 and 6.2% (91/1477) in Nepal, but higher than reported fatality rate of 1.5 (93 deaths /6224) in Bangladesh from 2004-2008 and 2.4% (853 deaths/34,918) in India.
In South Sudan community based longitudinal study showed that there was 20% case fatality rate of visceral leishmaniasis. Of the total reported treatment exited cases of 2263 patients ,2096 were cured. The total cure rate of kalazar patients in the period of 2009-2015 reported was 92.6% (2096/2263, report of 2009-2015). This cure rate was higher than that of Amhara region which was 90% reported from 1998-2003 [
6]. The highest cure rate was 90% in 2015, and the lowest was 89 % in 2009.
Discussion
On average 13 person (92/2263) per year died of visceral leishmaniasis within 7 years among kalazar patients exited at MSF Abderafi kalazar treatment center in West Armachiho district. The VL fatality rate reported by MSF Holland at Abdurafi kalazar treatment center was 4% (92/2263) cases from 2009-2015, which was lower than hospital-based of 7.2% in Brazil in 2006 and 6.2% (91/1477) in Nepal, but higher than reported fatality rate of 1.5 (93 deaths /6224) in Bangladesh from 2004-2008 and 2.4% (853 deaths/34,918) in India [7]. (And also in MSF Abdurafi kalazar treatment center in West Armachiho district the highest case fatality rate reported in the study period (2009-2015) was 7.4% which was lower than a community based longitudinal study in South Sudan which showed that 20% case fatality rate of visceral leishmaniasis. The total case fatality rate in this study was lower as compared with a retrospective cohort study conducted in Tigray, Ethiopia which showed that the case fatality rate of 18.5% [8] and a retrospective hospital based study conducted in North West Ethiopia (2013) which showed that 12.4% case fatality rate of VL [9]. The total cure rate of kalazar patients in the study period (2009-2015) at MSF Abderafi kalazar treatment center in West Armachiho district was 92.6 % (2096/2263).
This cured rate was higher than kalazar cured rate of 90% which reported by Amhara region from 1998 to 2003 years [
10]. In MSF Abderafi kalazar treatment center the highest and the least cured rate in the study period (2009-2015) were 96% and 89% in 2015 and 2009 respectively, which was higher than the highest and the least kala-azar cure rate of 94% and 70% in 2006 and 2008 respectively reported by Amhara region [
10].
In this study, the total Kala-azar/HIV co-infected was 12%. This was lower than 41% (87/212) visceral leishmaniasis cases tested for HIV and were co-infected in a study conducted at Gondar university hospital, northwest Ethiopia in 1999-2004 [
11].
The prevalence of VL-HIV co-infection in MSF Abdurafi treatment center, West Armachiho district was higher than 10.4% of a cross sectional study conducted in North West Ethiopia in 2014. [
12].
Limitation of the study
Variables related with sex and age of the patient were not reported. The kala-azar prevalence rate was not calculated because population denominator was not stable.
Conclusion
Visceral leishmaniasis was highly prevalent in the area. There was high kala-azar mortality rate and majority of deaths were unrecognized. Prevalence rate of VL-HIV co-infection and relapse was higher at MSF Abdurafi kalazar treatment center in West Armachiho district.
Recommendation
Ministry of health should strengthen prevention and control mechanisms of kala-azar. Ministry of health and MSF Holland should conduct further studies on the cause of death among kalazar patients, because there may be drug toxicity or other complications.
What is known about this topic
- The risk factors associated for visceral leishmaniasis prevalence and incidence in Ethiopia.
What this study adds
- This study adds information regarding the outcome of a seven year visceral leishmaniasis trend in the study area
- This study also utilized routine surveillance data to estimate trends and rates (mortality) which inform interventions and surveillance data collection, analysis and reporting systems.
Competing interests
The authors declare no competing interests.
Authors' contributions
Sisay Awoke designed of the study, collected, analyzed and wrote the documented Sefonias Getachew, Mr. Yimer Seid and Dr. Tatek Bogale participated in review and improve manuscript preparation. All authors read and approved the final manuscript.
Acknowledgments
First and most, we would like to express great appreciation and thanks to Dr. Sefonias Getachew and Mr. Yimer Seid for their constructive, unlimited and priceless comments and reviewing the manuscript. Secondly we would like to thank AAU programme coordinators and facilitators Dr. Adamu Addisie and Mrs. Abigiya Wondimagegnehu for making the programme favorable condition and successful practical application of the field. We heartedly thank Dr. Tatek Bogale Anbessie EFELTP country director and EPHA for financing and offering technical support to the programme.
Figures
Figure 1: Trend of kalazar screening and number of positives by year West Armachiho district, North Gondar zone, Amhara, Ethiopia, 2009-2015
Figure 2: Trend of primary kalazar and relapse among positives by year in West Armachiho district, North Gondar zone, Amhara, Ethiopia, 2009-2015
Figure 3: Trend of cure rate, positive rate and relapse rate of kalazar patients by year in West Armachiho district, North Gondar Zone, Amhara, Ethiopia, 2009-2015
Figure 4: Trend of mortality rate of kalazar in West Armachiho district, north Gondar Zone, Amhara, Ethiopia, 2009-2015
Figure 5: Rate of HIV/ Kalazar co-infection in West Armachiho district, Amhara region, Ethiopia, 2016
References
- Eds: Dan L. Longo, Anthony S. Fauci, Dennis L. Kasper, Stephen L. Hauser, J. Larry Jameson and Joseph Loscalzo. Harrison ‘s Principle of Internal Medicine. 18th ed. volume New York: McGraw Hill; 2012. Google Scholar
- John TD, Petri AW, Markell KE, Voge M. Markell and Voge's medical parasitology. 9th ed. Missouri: Saunders/Elsevier Inc; 2006. p 127-139.
- McGwire BS, Satoskar AR. Leishmaniasis: clinical syndromes and treatment. QJM. 2014 Jan; 107(1):7-14. https://doi.org/10.1093/qjmed/hct116 PubMed | Google Scholar
- Mondal D, Khan MG. Recent advances in post-kala-azar dermal leishmaniasis. Current opinion in infectious diseases. 2011 Oct 1; 24(5):418-22.https://doi.org/10.1097/qco.0b013e32834a8ba1 Google Scholar
- Barrett MP, Croft SL. Management of trypanosomiasis and leishmaniasis. Br Med Bull. 2012; 104(1):175-96. https://doi.org/10.1093/bmb/lds031 PubMed | Google Scholar
- WHO. Leishmaniasis in high-burden countries: an epidemiological update based on data reported in 2014. WHO. 201 Accessed May 2022. PubMed | Google Scholar
- Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J, Jannin J, den Boer M; WHO Leishmaniasis Control Team. Leishmaniasis worldwide and global estimates of its incidence. PLoS One. 2012;7(5):e35671.https://doi.org/10.1371/journal.pone.0035671 PubMed | Google Scholar
- Alvar J, Aparicio P, Aseffa A, Den Boer M, Cañavate C, Dedet JP, Gradoni L, Ter Horst R, López-Vélez R, Moreno J. The relationship between leishmaniasis and AIDS: the second 10 years. Clin Microbiol Rev. 2008 Apr;21(2):334-59https://doi.org/10.1128/CMR.00061-07 PubMed | Google Scholar
- Welay GM, Alene KA, Dachew BA. Visceral leishmaniasis treatment outcome and its determinants in northwest Ethiopia. Epidemiol Health. 2016 Dec 28; 39:e2017001.https://doi.org/10.4178/epih.e2017001 PubMed | Google Scholar
- ter Horst R, Collin SM, Ritmeijer K, Bogale A, Davidson RN. Concordant HIV infection and visceral leishmaniasis in Ethiopia: the influence of antiretroviral treatment and other factors on outcome. Clinical Infectious Diseases. 2008 Jun 1; 46(11):1702-9.https://doi.org/1086/587899 Google Scholar
- Mengistu G, Ayele B. Visceral Leishmaniasis and HIV co-infection in patients admitted to Gondar university hospital, northwest Ethiopia. The Ethiopian Journal of Health Development [Internet]. 2007 [cited 2022 May 25];21(1):53–60.
- Mengesha B, Endris M, Takele Y, Mekonnen K, Tadesse T, Feleke A, Diro E. Prevalence of malnutrition and associated risk factors among adult visceral leishmaniasis patients in Northwest Ethiopia: a cross sectional study. BMC Res Notes. 2014 Feb 4; 7:75.https://doi.org/10.1186/1756-0500-7-75 PubMed | Google Scholar