Trends of Injuries due to Gender Based Violence, Uganda, 2012 - 2016, a retrospective descriptive analysis
Claire Biribawa1,&, Rebecca Nuwemastiko2, Frederick Oporia2, Ezekiel Baguma3, Lilian Bulage1, Denis Okethwangu1, Alex Riolexus Ario1, Olive Kobusingye2
1Uganda Public Health Fellowship Program, Kampala, Uganda, 2Department of Disease control and Environmental Health, School of Public Health, Makerere University College of Health Sciences, Kampala, Uganda, 3Department of Surgery, College of Health Sciences, Makerere University, P.O Box 7072, Kampala, Uganda
&Corresponding author
Claire Biribawa, Uganda Public Health Fellowship Program, Kampala, Uganda. biribawaclaire@musph.ac.ug
Introduction:
Gender-based violence (GBV) in Uganda is widespread. The 2012 Uganda Bureau of Statistics report indicated that 60% of Ugandan women experienced GBV, which is approximately twice the global rate. There is paucity of information on epidemiology of injuries due to GBV in Uganda. We studied trends and distribution of injuries due to GBV in Uganda.
Methods:
We conducted a retrospective descriptive analysis using routinely-collected surveillance data from the Uganda Health Management Information System over five years (2012–2016). We calculated prevalence and annual injury rates due to GBV per 10,000 population and compared them across different population segments and time periods. We used logistic regression to determine trends.
Results:
In 2016, GBV resulted in 49,842 hospital visits in Uganda. Injury rates due to GBV were 13.5 per 10,000 population for the year 2012, and 13.6 per 10,000 population for 2016. Injury rates declined slightly from 2012 to 2016 (OR: 0.995, 95% CI: 0.991–0.997). In 2016, the odds of injuries due to GBV were 1.36 times in females compared to males (OR: 1.36, 95% CI: 1.33–1.38). Northern and Eastern regions (17.4 and 16.9 per 10,000, respectively) had higher GBV-associated injury burden than Central and Western regions (11.0 and 10.1 per 10,000 population, respectively).
Conclusion:
The incidence of injuries due to GBV in Uganda has not changed meaningfully from 2012 to 2016. We recommend development of interventions for GBV prevention targeting both males and females. There is a need for targeted efforts in the Eastern and Northern region.
Introduction

Violence is defined as the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation [1]. Gender-based violence (GBV) refers to violence perpetrated against a person´s will based on gender norms and unequal power relationships between two genders, within the context of a specific society [2]. It may include domestic abuse, sexual assault, child sexual abuse, sex trafficking, and certain traditional practices such as female genital mutilation [2].
All age groups and genders are affected by GBV, although women, girls, and children are most at risk [
3]. According to WHO global estimates, about one in three women have experienced some form of GBV in their lifetime [
4]. Gender based violence usually happens in the framework of family, community, work, and institutions, which are the places where people should be safe and protected [
5,
6].
GBV has profound health implications, affecting one´s physical, mental, sexual, and reproductive health, and often leads to injuries, disability, and sometimes death. Injuries resulting from GBV can translate into massive medical costs, with other economic losses involved due to loss of productivity [
4]. However a lack of reliable statistics on GBV-related injuries has largely hidden the health and economic impacts of these injuries. A systematic review carried out by World Health Organization (WHO) in 2013 revealed that 42% of all women who experienced physical and/or sexual violence by an intimate partner sustained some form of injury [
7].
The 2012 Uganda Bureau of Statistics report indicated that about 60% of women of reproductive age had ever experienced physical violence since age 15; this is almost twice the global rate [
8]. Physical violence during childhood was reported in 59% males and 68% males aged 18 - 24 years[
9].
Factors associated with the burden and perpetuation of GBV in Uganda may include weak policies preventing GBV, poor law enforcement against reported cases of GBV, low educational status, cultural beliefs about the normality of GBV, poverty, attitudes, and alcohol abuse [
2,
10]. A higher burden of GBV in areas of armed conflict has been documented in various national contexts, including in Northern Uganda [
10], which has been reported to have a heightened burden of GBV.
In Uganda, GBV data are captured in one of two ways. First, police may capture these data when they are reported: the Uganda Police Force has had a Gender desk since 1986 which was later incorporated into the Child and Family Protection Unit [
11]. Laws and regulations about GBV in Uganda include provisions for addressing assaults causing bodily harm and the relief and protection of victims of domestic violence. The second way GBV data are reported are from health facilities: all persons who report to health facilities with injuries must be asked about the source of their injuries. Those that are reported as arising from any form of GBV are categorized as '2018Injuries due to GBV' in the Uganda Health Management Information System (HMIS).
Although data on injuries due to GBV are captured in HMIS, data concerning these injuries have not been analyzed and published. The limited epidemiologic data and information on the burden of injuries due to GBV hampers the understanding required to put in place health policies and guidelines for appropriate interventions [
6,
8]. We determined the trends of injuries due to GBV and characterized the burden from 2012 to 2016 in Uganda using data from HMIS in order to inform interventions.
Methods

Study setting
We conducted the study in Uganda. Uganda is divided into four administrative regions: Central, Western, Northern, and Eastern, which are further sub-divided into 127 districts.
Study design
We conducted an analysis of routine secondary data reported through the Uganda Health Management Information System (HMIS). The analysis involved all persons presenting to health facilities with injuries due to GBV from the year 2012-2016. We defined injuries due to GBV as a clinician diagnosis of any physical damage to the body resulting from any act that is perpetrated against a person´s will based on gender norms or unequal power relations [
2].
Data sources
The HMIS is an integrated reporting system used by the Ministry of Health Uganda, development partners, and stakeholders to collect health information on a routine basis. HMIS data are used to monitor the Health Sector Strategic Plan (HSSP) indicators to enable planning, decision-making, monitoring, and evaluation of the healthcare delivery system. Information in HMIS is collected on a routine basis from every health unit in all districts within Uganda. HMIS information flows from the lowest level (the community) to the health unit (Health Center Two, Three, and Four-level facilities, General Hospitals, and referral hospitals), health sub-district, district, and finally to the National Health Databank at the Resource Centre of the Ministry of Health
Figure 1. Electronic HMIS (DHIS) is a platform for reporting, analysis and dissemination of health data reported through the HMIS. Within the DHIS, data on injuries due to GBV are aggregated by age, sex, location of reporting, and time. We analyzed data on all injures due to GBV submitted to the HMIS during 2012-2016. We abstracted and analyzed data on sex, district, and administrative region where these injuries were reported.
Data management and analysis
We used MS Excel version 2010 for data cleaning and analysis. We abstracted data on a monthly basis. We used univariate analysis to obtain frequencies for sex, regions, and years. For regional distribution characteristics of the injuries due to GBV, we ran frequencies based on the location of the health facilities where the patients sought care.
We calculated incidence of injuries due to GBV using the 2014 population estimates from the Uganda Bureau of Statistics [
12]. We calculated overall district-specific incidence rates, which were then exported to QGIS version 2.8 to produce a choropleth map based on the Uganda 2014 district shape files for the most recent year, 2016. We also calculated institutional prevalence of injuries due to GBV based on numbers of OPD visits per year. We conducted trend analysis, for the injuries due to GBV for the whole country and in the various administrative regions using Epi-Info version 7.2. We ran a logistic regression test for assessing trends to determine if a statistically significant change occurred over time [
13].
Ethics approval and consent to participate
Administrative authorization to access the data was received from the Uganda Ministry of Health. In addition, the Office of the Associate Director for Science, CDC Uganda, determined that this activity was not human subjects´ research, as its primary intent was to improve public health practice. Data abstracted did not include personal identifiers.
Results
The institutional proportion of outpatient visits due to GBV-associated injuries ranged from 0.12% (2016) to 0.14% (2012) Table 1. Injury rates due to GBV were 13.5 per 10,000 population in 2012, and 13.6 per 10,000 population in 2016. Trends in the rates of injuries due to GBV remained constant from 2012 to 2016 (OR: 0.995, 95% CI: 0.991 - 0.997). Across the 5 years, females were more affected by injuries due to GBV compared to males. The odds of injuries due to GBV among females compared to males were OR= 1.38 in 2012, OR= 1.49 in 2013, OR= 1.42 in 2014, OR= 1.41 in 2015 and OR= 1.36 in 2016 Table 2.
Among the four regions (Northern, Central, Eastern and Western regions), the Northern region had the highest incidence of injuries due to GBV throughout the 5 year period
Figure 2. In 2016, the rate of injuries due to GBV was 17.4 per 10,000 population in the Northern region, 16.9 per 10,000 in the Eastern region, 11.0 per 10,000 in the Central region, and 10.1 per 10,000 in the Western region. Based on the trend analysis, there was a 5% annual decline (OR: 0.95, CI: 0.947-0.96) in the burden of injuries due to GBV over the 5-year period in the Northern region and 4% annual reduction (OR: 0.96, CI: 0.95-0.97) in the Western region. In contrast, there was an annual increase of 2% in the burden of injuries due to GBV in the Eastern and Central regions over the 5-year period (OR: 1.02, CI: 1.018-1.03 and OR: 1.02, CI: 1.01 - 1.03, respectively).
There was no clear seasonality from the monthly pattern in the number of injuries due to GBV reported. However, the early and later months of the year see raised numbers of injuries due to GBV. The high numbers were especially reported in the month of March and December
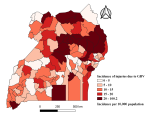
Figure 3. The burden of injuries due to GBV varied by district, but specific districts in the Northern region had the highest rates. Districts in the Northern region with higher incidences of injuries due to GBV included Moyo, Adjuman, Lamwo, Kitgum, Moroto, Napak, Nakapiripiti, Amuria, Katakwi, Otuke, Lira, Oyam, Apac, Kole, and Alebtong (incidence rate: 18.9-100.2 per 10,000 population
Figure 4.
Discussion
The trend of injuries due to GBV in Uganda remained constant from 2012 to 2016. Injuries due to GBV were prevalent countrywide, but districts in the northern region were the most affected.
In Uganda, there are provisions that address GBV in the 1995 Constitution of Uganda which include the Penal code Act CAP 120, with provisions addressing assaults causing bodily harm, and the Domestic Violence Act of 2010, which provides for the protection and relief of victims of domestic violence, the punishment of perpetrators, and judicial procedures and guidelines. However, these have not seen much success [
14]. The sustained high incidence of injuries due to GBV is at least in part attributed to the way GBV is deeply entrenched in some cultural practices regarding intimate relationships in Uganda [
14].
There was some kind of seasonality in the pattern of injuries due to GBV with raised numbers in the early and later months of the year. Studies have reported that seasonality of GBV have patterns that are associated with weather, climate, agriculture or economic cycles. Reported GBV has been linked to the agricultural season with higher rates during the planting and harvest seasons, while violence against children at the start of the agricultural year. During the rainy season, there is increased GBV as decisions are made on how to utilize meager resources [
15,
16].
The 13.6 per 10,000 population incidence of injuries due to GBV in Uganda was high and yet this only highlights the greater underlying burden, for it is vastly under-reported [
17]
The incidence of physical injuries due to GBV was more predominant in the Northern compared to other regions. This is similar to what was reported in the Uganda Demographic Health Survey (UDHS) of 2011, where the Northern and Eastern regions had higher incidences of GBV compared to other regions [
8]. In the Northern region, districts that had high incidences of injuries due to GBV included Adjuman, Kitgum, Lamwo, and Lira. These are the districts that had previous war conflict from the Lord´s Resistance Army rebels. In addition, refugees flock in large numbers to the Northern region of Uganda due to the civil unrest in South Sudan. Stewart and Brown reported higher incidence of GBV in areas that had been affected by civil or ethnical unrest [
18]. Previous experience of violence has been reported to be a risk factor for perpetrating violence to others [
4]. There is therefore need to explore the burden of GBV in these communities in order to clearly identify risk factors and so design targeted interventions.
Our analysis revealed that females reported more GBV-associated injuries compared to males. Although documentation of GBV among men is unusual, it is not unheard of [
19]. Many of these may be in male children; the broad age categories available for the data in this study did not allow us to evaluate whether or not these were primarily in children. A report on violence against children in Uganda reported that significantly more boys than girls experienced physical violence [
9]. We recommend further research into this issue, focusing on the burden of injuries due to GBV among males, the ages at which it occurs, and the forms of injuries sustained in Uganda.
Unfortunately, HMIS data lacked information on the triggers of GBV, the type of injury sustained, and the relationship with the perpetrators of GBV, which would inform prevention measures. In addition, some variables such as age were aggregated into very large categories (≤5 years and >5 years), making more detailed analysis by smaller age group impossible. There was almost certainly underestimation of the prevalence of injuries due to GBV, because only a small proportion of affected persons ever report to formal healthcare sites [
20-22] and health care workers may not record the relationship of the injury due to GBV especially in cases of males. In addition the prevalence could be varied among population segments due to differences in health seeking behaviors for example the varying differences between males and females.
We propose further research to evaluate the prevention efforts and interventions currently in place against GBV in Uganda. The high and consistent rates of GBV indicate a need for continuous assessment, monitoring, and documentation of injuries due to GBV in Uganda to indicate the effectiveness of interventions that are in place. Beyond this, additional analyses about types of GBV injuries by sex and qualitative research on the circumstances surrounding such injuries will be helpful in designing preventive interventions.
Conclusion
The incidence of injuries due to GBV in Uganda has remained stable from 2012 to 2016. The Northern region of Uganda shares a disproportionate burden of injuries due to GBV compared with other regions. Injuries due to GBV affected more females than males. Prevention and control measures on GBV may need to be targeted towards all persons, and not just women and children.
What is known about this topic
- This study assessed a five year trend of injuries due to Gender Based Violence however what has been previously known is the burden of gender based violence as highlighted from the Uganda Demographic Health Survey. In addition risk factors and triggers for gender based violence have been documented in various research articles.
What this study adds
- This study adds information regarding the incidence of injuries due to gender based violence in Uganda and a report on a 5 year trend analysis of injuries due to gender based violence in Uganda.
- This study also utilized routine surveillance/ HMIS data to estimate the trends and rates. This highlights the importance of using routinely collected data to inform and guide development of interventions and also improve the data collection systems.
Competing interests
The authors declare no competing interests.
Funding
This project was supported by the President´s Emergency Plan for AIDS Relief (PEPFAR) through US Centers for Disease Control and Prevention under the terms of Cooperative Agreement number GH001353-01 through Makerere University School of Public Health to the Uganda Public Health Fellowship Program, Ministry of Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official positions of the US Centers for Disease Control and Prevention, Makerere University School of Public Health, or the Ministry of Health.
Authors' contributions
CB Led the designing of the study, abstracting data from the HMIS, and subsequent analysis. CB wrote the drafts of the manuscript and revised the paper for substantial intellectual content. ARA, RN, LB, EB, FO, DO and OK participated in the design and analyses of the study and reviewed the draft manuscript, providing substantial intellectual involvement. All authors read and approved the final manuscript.
Acknowledgements
The authors thank the Division of Health Information, Ministry of Health Uganda which facilitated the capture and data abstraction for this study. We acknowledge the African Field Epidemiology Network (AFENET) and Makerere University School of Public Health for facilitating a one-week technical manuscript-writing workshop in which the first draft of this manuscript was developed. We also acknowledge AFENET, the Makerere University School of Public Health, and the US CDC for the technical guidance during the development of this manuscript.
Tables and figures
Table 1: Number of Outpatient department visits and institutional rates for injuries due to GBV, Uganda, 2012 - 2016
Table 2: Distribution of injuries due to GBV based on sex, Uganda, 2012-2016
Figure 1: Information flow in the Health Management Information System
Figure 2: Trends of injuries due to GBV disaggregated by regions, Uganda, 2012-2016
Figure 3: Monthly patterns of injuries due to GBV
Figure 4: District specific incidences for injuries due to GBV, Uganda, 2016
References
- Krug EG, Mercy JA, Dahlberg LL, Zwi AB. The world report on violence and health. The Lancet. 2002;360(9339):1083-1088. https://doi.org/10.1016/S0140-6736(02)11133-0. Google Scholar
- Bloom SS. Violence against women and girls: a compendium of monitoring and evaluation indicators.Measure Evaluation. 2008. Accessed May 2020.
- Gurman TA, Trappler RM, Acosta A, McCray PA, Cooper CM, Goodsmith L. 'By seeing with our own eyes, it can remain in our mind': qualitative evaluation findings suggest the ability of participatory video to reduce gender-based violence in conflict-affected settings. Health Educ Res. 2014;29(4):690-701.https://doi.org/10.1093/her/cyu018. Google Scholar
- World Health Organization. Violence against women. WHO. 2017. Accessed September 2018.
- Butchart A, Mikton C. Global status report on violence prevention, 2014. WHO. 2014. Google Scholar
- Hofman K, Primack A, Keusch G, Hrynkow S. Addressing the growing burden of trauma and injury in low-and middle-income countries. Am J Public Health. 2005; 95(1):13-17.https://doi.org/10.2105/AJPH.2004.039354 . PubMed | Google Scholar
- World Health Organization. Violence against women: a 'global health problem of epidemic proportions'. WHO. 2013. Accessed May 2020.
- UBOS and Calverton, Maryland: ICF International Inc. Uganda demographic and health survey 2011. UBOS. 2012. Accessed May 2020. Google Scholar
- Ministry of Gender, Labour and Social Development (MGLSD). Uganda Violence Against Children Survey; key findings. UNICEF. 2018.
- Akumu CO, Amony I, Otim G. Suffering in silence: a study of sexual and gender based violence (SGBV) in Pabbo camp Gulu district northern Uganda. 2005. Accessed June 2019.
- Namanya B. Spousal assault and the Child and Family Protection Unit (CFPU) of the Uganda Police Force. Police Pract Res. 2008;9(1):31-41.https://doi.org/10.1080/15614260801969912 . Google Scholar
- Uganda Bureau of Statistics. The national population and housing census 2014-main report. Uganda Bureau of Statistics. 2016. Accessed March 2019.
- CDC. Interpretation of YRBS trend data. CDC. 2016.
- Mbonye M, Nalukenge W, Nakamanya S, Nalusiba B, King R, Vandepitte J, et al. Gender inequity in the lives of women involved in sex work in Kampala, Uganda. J Int AIDS Soc. 2012; 15(Suppl 1): 17365. https://doi.org/10.7448/IAS.15.3.17365. PubMed | Google Scholar
- FAO. Guidance note: Gender-Based Violence and Livelihood Interventions. FAO. Accessed May 2019.
- NFPA. Evaluation of UNFPA support to the Prevention, Response to and Elimination of Gender Based Violence and Harmful practices; 2012 -2017, Uganda Case Study. 2018.
- Palermo T, Bleck J, Peterman A. Tip of the Iceberg: Reporting and Gender-Based Violence in Developing Countries. Am J Epidemiol. 2014;179(5):602-12.https://doi.org/10.1093/aje/kwt295 . PubMed | Google Scholar
- Stewart F, Brown G, Mancini L. Monitoring and measuring horizontal inequalities. Centre for Research on Inequality, Human Security and Ethnicity. 2010;4. Google Scholar
- Oladepo O, Yusuf OB, Arulogun OS. Factors influencing gender based violence among men and women in selected states in Nigeria. Afr J Reprod Health 2011;15(4):78-86.
- Hyman I, Forte T, Mont JD, Romans S, Cohen MM. Help-seeking rates for intimate partner violence (IPV) among Canadian immigrant women. Health Care Women Int 2006;27(8):682-694.https://doi.org/10.1080/07399330600817618 . Google Scholar
- Langton L, Berzofsky M, Krebs CP, Smiley-McDonald H. Victimizations not reported to the police, 2006-2010. US Department of Justice, Office of Justice Programs, Bureau of Justice Statistics Washington, DC. 2012. Accessed November 2018. Google Scholar
- Casey SE, Gallagher MC, Makanda BR, Meyers JL, Vinas MC, Austin J. Care-seeking behavior by survivors of sexual assault in the Democratic Republic of the Congo. Am J Public Health 2011;101(6):1054-1055. https://doi.org/10.2105/AJPH.2010.300045. PubMed | Google Scholar