Characteristics of homeless people screened for SARS-CoV-2, Harare, Zimbabwe 2021
Takudzwa Marembo1,2,&, Tendai Chipendo1, Stanford Chigaro3, Portia Manangazira1,4, Donewell Bangure1
1Africa Centres for Disease Control and Prevention, African Union Commission, Roosevelt Street (Old Airport), Addis Ababa, P.O. Box 3243, Addis Ababa, Ethiopia, 2Department of Medical Microbiology, Midlands State University Faculty of Medicine, Gweru, Zimbabwe, 3Public Health Institute, Texila American University, Harare, Zimbabwe, 4Ministry of Health and Child Care, Epidemiology and Disease Control Directorate, Harare, Zimbabwe
&Corresponding author
Marembo Takudzwa, Africa Centre for Disease Control and Prevention, African Union Commission, Roosevelt Street (Old Airport), Addis Ababa, Ethiopia. temkanya@gmail.com
Introduction:
During the COVID-19 pandemic, homeless people in Zimbabwe were being shifted to rehabilitation centres awaiting transportation to their place of origin. The homeless people were firstly screened for SARS-CoV-2 such that infected individuals were isolated from uninfected ones to prevent in-shelter transmission. This study analysed the characteristics of homeless people who were screened for SARS-CoV-2 in Harare.
Methods:
A retrospective cross-sectional study of secondary SARS-CoV-2 data from homeless people tested at Africa Institute of Biomedical Science and Technology (AiBST) laboratory; Harare in January 2021 was done. Epi Info TM 7.2.2.6 was used to to generate frequencies, measures of central tendency and proportions of the different characteristics of the SARS-CoV-2 records. Bivariate analysis was used to estimate the association of the demographic characteristics with the outcome of interest (SARS-CoV-2 positive diagnosis).
Results:
One hundred and six homeless people were tested for SARS-CoV-2 and 85% (90/106) were males. Twenty-five percent (27/106) of the study participants tested positive for SARS-CoV-2. Eighty-one percent (22/27) of the SARS-CoV-2 infected cases were males. Participants in the 0-20yr age group were 2.49 times (p <0.05; OR = 1.01 - 6.14) at risk of being SARS-CoV-2 infected than those above 21years. Eighty-one percent (22/27) of the SARS-CoV-2 cases were asymptomatic.
Conclusion:
SARS-CoV-2 infections were found in homeless people from the streets of Harare. There is need to conduct regular SARS-CoV-2 screening among this population regardless of the symptom status since majority of the infected cases were asymptomatic.
Introduction

Coronavirus disease 2019 (COVID-19) is a communicable respiratory disease caused by a novel coronavirus called Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) [1]. The initial cases of COVID-19 were identified in Wuhan City, Hubei Province, China and reported to the World Health Organisation (WHO) on December 31, 2019 [1]. Since then, the disease has spread to almost every region and country in the world and was declared a COVID-19 a global pandemic by the WHO on March 11, 2020 [2].
Over 100 million cases have been reported globally with approximately two million deaths as of 28 January 2021 [
2]. Zimbabwe recorded its initial case on the 20th of March 2020 and there was gradual increase in the number of cases up to July 2020. The country experienced an upsurge of cases in August 2020, from 3659 to 6497 from the 1st to the 31st of August [
3]. The case fatality ratio also increased from 1.8% to 3.1% during the same period. There was a steady increase in the number of cases in the following months from September to December [
3].
Since the beginning of 2021, there has been a surge of cases and deaths in what is believed to be the second wave of the pandemic. As of 28 January 2021, the number of cases and deaths were 32 646 and 1160 respectively with a case fatality ratio of 3.5% [
3].
Various mitigation strategies have been taken to limit the spread of SARS-CoV-2 infections in the country. These include complete or partial lockdowns, travel bans, mass gathering restrictions, home quarantines within communities, social distancing measures and personnel protective actions.
Although the main symptoms of COVID-19 include fever, cough, respiratory difficulties, up to severe complications such as acute respiratory distress syndrome, a large portion of cases are asymptomatic [
4]. Asymptomatic carriers account for about 40% of COVID-19 cases and are characterized by the absence of symptoms but having the same infectivity as symptomatic infections [
5]. Furthermore, asymptomatic cases can lead to significant subclinical lung abnormalities in a short time, suggesting that the absence of symptoms may not imply the absence of harm [
6].
The large number of asymptomatic patients is an extremely important characteristic of SARS-CoV-2 infection; however, it becomes even more important in settings with specific vulnerabilities, such as among homeless people living on the streets, where the consequences on individual and public health may be dramatic [
4]. Homeless people are a population group of great social vulnerability, heterogeneous, with characteristics related to extreme poverty, interrupted or weakened family ties, without regular conventional housing, which uses public places and/or degraded areas, either temporarily or permanently [
7].
In Harare, these homeless people mostly children and youths, are spread across the city, sharing space in alleyways, market places, low-income settlements, or on wasteland. Their sources of income include picking plastics for recycling and begging for money from motorists at robots [
8]. The problem of living on the street is crossed daily by proliferation of diseases, violence, stress and hostility. Getting sick on the streets has its own characteristics in the health-disease process, being determined by spacing between meals, exposure to climate change and other factors [
9,
10].
Considering the constant movement of these people in search for food, often found in bins and their frequent interaction with people while begging for food and money, there is a high risk of acquiring COVID-19 among this group and transmission to the general population. This is also coupled with limited use of face masks, and often precarious hygienic conditions in the streets. There is limited literature on the burden of COVID-19 among the vulnerable groups, particularly people living in the streets in Zimbabwe. During the COVID-19 pandemic, homeless people were being shifted to rehabilitation centres awaiting transportation to their place of origin. Regardless of the symptom status, the homeless people were screened for SARS-CoV-2 such that infected individuals were isolated from uninfected ones to prevent in-shelter SARS-CoV-2 transmission. We therefore analysed the SARS-CoV-2 testing data collected from homeless people in January 2021 at AiBST laboratory in Harare.
Methods

Study design
A retrospective cross-sectional study based on secondary COVID-19 data from AiBST laboratory in Harare was done.
Study Setting
This is the period when Zimbabwe experienced its second wave of SARS-CoV-2. The laboratory is one of the major research and education institutes in Zimbabwe carrying out a wide range of activities ranging from molecular diagnostics to forensic science. The laboratory´s main catchment area is Harare, with a population of approximately two million people basing on the 2012 census projections. There is an adequate staff complement of proficient scientists with great capacity for quality testing and an electronic information system to store and manage data. The laboratory receives COVID-19 specimens for Reverse Transcriptase Polymerase Chain Reaction (RT PCR) from both private and public health institutions across Zimbabwe.
Data source
The COVID-19 data from the laboratory request forms were captured and stored in the Laboratory Information Management System (LIMS). The dataset included information on COVID-19 testing results, categorised as positive and negative, date of specimen collection, specimen originating site, date of result dispatch as well as individual level data on demographic characteristics and facility specific information and clinical characteristics. Demographic information included patients´ age and gender. The dataset was created and analysed in January 2021.
Study variables
As per the country COVID-19 laboratory policy, the laboratory was expected to perform RT-PCR assays for the detection of SARS-CoV-2. The outcome variable of interest in the study was whether a patient was diagnosed with SARS-CoV-2 infection or not, defined as a dichotomous indicator.
Data analysis
Data quality was checked using completeness of data entries in LIMS. Epi InfoTM 7.2.2.6 software was used to generate frequencies, measures of central tendency and proportions of the different characteristics of the COVID-19 records. To estimate the association of the demographic characteristics with the outcome of interest (SARS-CoV-2 positive diagnosis for all patients), we conducted bivariate analysis using the same software.
Study subjects and sample collection
The data was collected from the 4th to the 29th of January 2021 in Zimbabwe. The study subjects were homeless people relocated from the streets of Harare, to three different shelter homes namely Beatrice Rehabilitation Centre, Mt Hampden Youth Vocational Training Centre and Ruwa Rehabilitation Centre awaiting transportation to their place of origin. The Zimbabwean Ministry of Public Service, Labour and Social Welfare, Harare province sanctioned the testing of these homeless people as a way of preventing shelter-based outbreak by isolating infected individuals. The Ministry of Health and Child Care Zimbabwe laboratory request form was used for collection of demographics (age, sex), symptom status, date of sample collection and type of sample collected. The data were captured in the Laboratory Information Management System (LIMS).
Data analysis
The primary outcome was SARS-CoV-2 infection, defined as detection of SARS-CoV-2 from a nasal swab, regardless of symptoms. The COVID-19 data from the Laboratory Information Management System were transferred into Epi-Info
™ 7- (CDC, 2012) statistical package which was used for statistical analysis. The p-values < 0.05 were considered statistically significant.
Ethical Considerations
Permission to access the data was given the management of AiBST laboratory. The names of SARS-CoV-2 patients were not captured. An anonymous identification number was assigned to each record during data analysis. Adequate administrative authorization was obtained to conduct the study.
Results
Demographic Characteristics
One hundred and six homeless people were screened for SARS-CoV-2. Eighty- five percent (90/106) were males. Forty-eight percent (51) of the homeless people were in the 11 to 20-year age group while 37% (39) were in the 21-30 years age group. The median age of the study participants was 21 years. Most of the participants 58% (62) were from Mt Hampden rehabilitation centre. The demographic characteristics of the participants are as shown in
Table 1.
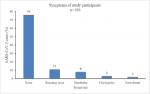
Symptoms Profile
Seventy-six percent (81/106) of the study participants did not present with any signs and symptoms. Eleven percent (12/106) presented with running nose, 8% (8/106) with headache, while 3% (3/106) had chest pains
Figure 1.
SARS-Cov-2 Infection status
Seventy-five percent (79/106) of the study participants tested negative for SARS-CoV-2, while 25% (27/106) tested positive.
Distribution of positive cases by sex and age group
Eighty-one percent (22/27) of the SARS-CoV-2 infected cases were males, while 19% (5/27) were females. Most of the study participants 63% (17/27) were in the 11 to 20-year age group, 30% (8/27) were in the 21-30 year age group, while 7% (2/27) were in the 31-40 age group
Figure 2.
Association between Demographic factors and Symptom profile with SARS-CoV-2 Infection Status
The risk of being infected with SARS-CoV-2 was higher in the younger age group. The participants in the 0 to 20-year age group were 2.49 times (p <0.05, OR=1.01-6.14) at risk of being SARS-CoV-2 infected than those above 21years. There was no association between being sex and SARS-CoV-2 infection status as well as symptom status and SARS-CoV-2 infection status
Table 2.
Discussion
SARS-Cov-2 was detected in 25% of the homeless people from the streets of Harare. The infections were most prevalent in the young population. This can be attributed to the fact that the younger population is the one which is most versatile and hence at more risk of acquiring the infections. SARS-CoV-2 infections being common in men than females as observed in this study can be as a result of overexpression of angiotensin converting enzyme (ACE) in men than females [11]. ACE is the receptor which facilitates SARS-CoV-2 entry into the cells. Consistent with our findings, available data from other countries show a SARS-CoV-2 infection prevalence of 11-30 % among the homeless [12-14]. Lewer et al (2020), however, expected SARS-CoV-2 infections to occur in 4% of the homeless people in modelling projections carried out by in England [15].
The occurrences of SARS-CoV-2 infections among the homeless are of importance for two major reasons. The first reason is that the homeless population can be key drivers of infection spread. The homeless population in Harare frequently interact with several people during their day-to-day activities which include car wash services, begging through the car windows, touting, among others. Due to unavailability of masks and hand sanitisers among this population, the chances of passing of the infection to others can be high. Spread of infections among the homeless can also happen faster due to poor sanitary conditions among the homeless. In as much as efforts are being made to relocate the homeless from the streets of Harare, some are finding their way back due to addiction to street life. This shows the need to focus on control measures targeting this population in curbing the spread of SARS-CoV-2. Some of the measures to undertake may include special hostels for the homeless, heath education and ensuring standard precaution measures targeting the homeless.
The second reason why it is important to protect the homeless is to shield them from devastating effects of SARS-CoV-2 infections. In as much as majority of the cases were asymptomatic, asymptomatic cases can lead to significant subclinical lung abnormalities in a short time, suggesting that the absence of symptoms may not imply the absence of harm [
6]. Furthermore, many people living on the streets already have diminished health condition, higher rates of chronic illnesses such as hypertension, cardiovascular disease or compromised immune systems, all of which increases risk for development of more serious manifestation of SARS-CoV-2 infection [
15-18]. Additionally, higher levels of drug and alcohol addiction common in the homeless worsen general health status [
19]. Due to social and economic factors, the access of screening and treatment services such as primary care clinics may be less accessible for these populations especially for those suffering from mental illness who may have difficulties in recognizing the threat of SARS-CoV-2 infection and its early symptoms.
In this study, majority of the infected were asymptomatic and there was no association between SARS-CoV-2 symptoms and SARS-CoV-2 infection status among homeless people in Harare. This is consistent with findings from a study by Ralli et al, 2020 were most of the positive cases (75%) were asymptomatic at the time of the testing and in the 14 days before, while only three patients had symptoms that included fever, diarrhoea, and cough [
6]. This highlights the need to conduct regular SARS-CoV-2 screening among this population regardless of the symptom status.
Conclusion
SARS-CoV-2 infections were found in homeless people from the streets of Harare. Screening for SARS-CoV-2 when moving homeless people to homeless shelters is necessary to prevent shelter-based outbreaks and symptoms status should not be used as a criterion for screening for SARS-CoV-2 among the homeless population. This study used convenient sampling which became a limitation of this study
What is known about this topic
- COVID ‐ 19 is a respiratory disease caused by SARS-CoV-2.
- People infected with SARS-CoV-2 can be asymptomatic or symptomatic.
- Homeless people are vulnerable population at risk of acquiring COVID-19
What this study adds
- The prevalence of SARS-CoV-2 among the homeless population in Harare
- The symptom profiling of SARS-CoV-2 infected people in Harare
- The association between demographic factors and symptom profile with SARS-CoV-2 infection status among the homeless people in Harare
Competing interests
The authors declare no competing interests.
Authors' contributions
TM and TC were responsible for the laboratory work and data acquisition and data analysis. TM, TC, PM, SC, DB participated in writing and review of the manuscript. All authors read and approved the final manuscript.
Acknowledgments
We would like to acknowledge the Africa CDC for providing reagents that were used in the testing for SARS-CoV-2 and African Institute for Biomedical Sciences and Technology (AiBST) for availing the equipment and infrastructure for laboratory work.
Tables and figures
Table 1: Demographic Characteristics of homeless people, Harare, 2021 (n=106)
Table 2: Demographic factors and Symptoms profile by SARS-CoV-2 Infection Status, Harare, 2021
Figure 1: Reported symptoms of study participants, Harare, 2021
Figure 2: Distribution of SARS-CoV-2 infected cases by age group, Harare, 2021
References
- World Health Organization.Origin of SARS-CoV-2 [Internet]. Geneva, Switzerland: World Health Organization; 2020 Mar 26 [cited 2023 Aug 7].
- World Health Organization.WHO Coronavirus Disease (COVID-19) Dashboard [Internet]. Geneva, Switzerland: World Health Organization; 2020 [cited 2021 Jan 28].
- Ministry of Health and Child Care.Zimbabwe Covid-19 SitRep, 28/01/2021 [Internet]. Harare, Zimbabwe: Ministry of Health and Child Care; 2021 Jan 28 [cited 2023 Jul 25].
- Kronbichler A, Kresse D, Yoon S, Lee KH, Effenberger M, Shin JI.Asymptomatic patients as a source of COVID-19 infections: A systematic review and meta-analysis . Int Journal Infect Dis [Internet]. 2020 Jun 17 [cited 2023 Jul 25];98:180-6. https://doi.org/10.1016/j.ijid.2020.06.052 PubMed | Google Scholar
- Chen T, Guo S, Zhong P.Epidemic characteristics of the COVID-19 outbreak in Tianjin, a well-developed city in China . American Journal of Infection Control [Internet]. 2020 Jun 12 [cited 2023 Jul 25];48(9):1068-73. https://doi.org/10.1016/j.ajic.2020.06.006 PubMed | Google Scholar
- Ralli M, Morrone A, Arcangeli A, Ercoli L.Asymptomatic patients as a source of transmission of COVID-19 in homeless shelters . International Journal of Infectious Diseases [Internet]. 2020 Dec 12 [cited 2023 Jul 25];103:243-5. https://doi.org/10.1016/j.ijid.2020.12.031 PubMed | Google Scholar
- Paula HC, Daher DV, Koopmans FF, Faria MGA, Lemos PFS, Moniz MA.Sin Aislamiento: Etnografía de las Personas Sinhogar en la Pandemia de COVID-19 [No Place to Shelter: Ethnography of the Homeless Population in the COVID-19 Pandemic] . Rev. Bras. Enferm [Internet]. 2020 [cited 2021 Jan 28];73(Suppl 2): e20200489. Spanish. https://doi.org/10.1590/0034-7167-2020-0489 Google Scholar
- Hunter J, van Blerk L, Shand W.Young people living on Harare´s streets provide glimpses into life under COVID-19 lockdown . The Conversation [Internet]. 2020 Sep 9 [cited 2023 Jul 25];Politics:[5 p.].
- Paiva IKSD, Lira CDG, Justino JMR, Miranda MGDO, Saraiva AKDM. Direito à saúde da população em situação de rua: reflexões sobre a problemática. [Homeless people's right to health: reflections on the problems and components] . Ciênc saúde coletiva [Internet]. 2016 Aug [cited 2023 Jul 25];21(8):2595-606. Portuguese. https://doi.org/10.1590/1413-81232015218.06892015 Google Scholar
- Karb R, Samuels E, Vanjani R, Trimbur C, Napoli A.Homeless Shelter Characteristics and Prevalence of SARS-COV-2 . WestJEM [Internet]. 2020 Aug 17 [cited 2023 Jul 25];21(5):1048-53. https://doi.org/5811/westjem.2020.7.48725 PubMed | Google Scholar
- Bwire GM. Coronavirus: Why Men are More Vulnerable to COVID-19 Than Women? SN Compr Clin Med [Internet]. 2020 Jun 4 [cited 2023 Jul 25];2(7):874-6. https://doi.org/10.1007/s42399-020-00341-w Google Scholar
- Mosites E.Assessment of SARS-COV-2 Infection Prevalence in Homeless Shelters- Four US Cities, March 27-April 15, 2020 . MMWR Morb Mortal Wkly Rep [Internet]. 2020 May 1 [cited 2023 Jul 25];69(17):521-2. https://doi.org/10.15585/mmwr.mm6917e1 PubMed | Google Scholar
- Baggett TP, Keyes H, Sporn N, Gaeta JM.Prevalence of SARS-COV-2 Infection in Residents of a Large Homeless Shelter in Boston . JAMA [Internet]. 2020 Apr 27 [cited 2023 Jul 25];323(21):2191-92. https://doi.org/10.1001/jama.2020.6887 Google Scholar
- Lewer D, Braithwaite I, Bullock M, Eyre MT, White PJ, Aldridge RW, Story A, Hayward AC.COVID-19 Among People Experiencing Homelessness in England: a modelling study . The Lancet Respiratory Medicine [Internet]. 2020 Sep 23 [cited 2023 Jul 25];8(12):1181-91. https://doi.org/10.1016/S2213-2600(20)30396-9 Google Scholar
- Rogers JH, Link AC, McCulloch D, Brandstetter E, Newman KL, Jackson ML, Hughes JP, Englund JA, Boeckh M, Sugg N, Ilcisin M, Sibley TR, Fay K, Lee J, Han P, Truong M, Richardson M, Nickerson DA, Starita LM, Bedford T, Chu HY. Characteristics of COVID-19 in Homeless Shelters: a Community-Based Surveillance Study . Ann Intern Med [Internet]. 2020 Sep 15 [cited 2023 Jul 25];174(1):42-9. https://doi.org/10.7326/M20-3799 Google Scholar
- Lima NNR, De Souza RI, Feitosa PWG, Moreira JLDS, Da Silva CGL, Neto MLR.People experiencing homelessness: their potential exposure to COVID-19 . Psychiatry Research [Internet]. 2020 Apr 11 [cited 2023 Jul 25]; 288:112945. https://doi.org/10.1016/j.psychres.2020.112945 PubMed | Google Scholar
- Ralli M, Cedola C, Urbano S, Morrone A, Ercoli L.Homeless Persons and Migrants in Precarious Housing Conditions and COVID-19 Pandemic: Peculiarities and Prevention Strategies . Eur Rev Med Pharmacol Sci [Internet]. 2020 Sep 30 [cited 2023 Jul 25];24(18):9765-7. https://doi.org/10.26355/eurrev_202009_23071 Google Scholar
- Tucker JS, D´Amico EJ, Pedersen ER, Garvey R, Rodriguez A, Klein DJ.Behavioral Health and Service Usage During the Covid-19 pandemic among Emerging Adults Currently or Recently Experiencing Homelessness . Journal of Adolescent Health [Internet]. 2020 Aug 10 [cited 2023 Jul 25];67(4):603-5. https://doi.org/10.1016/j.jadohealth.2020.07.013 PubMed | Google Scholar
- Peate I.Self-isolation and the Homeless Population . Br J Nurs [Internet]. 2020 Apr 11 [cited 2023 Jul 25];29(7):387. https://doi.org/10.12968/bjon.2020.29.7.387 Google Scholar