Children´s understanding of COVID-19 spread and its preventive strategies in Uganda: a cross sectional study among children aged 10 to 13 years in Hoima District
Christine Nalwadda Kayemba1,2, Lydia Kabwijamu3,2, Maxencia Nabiryo1, Andew Tusubira1, Justine Bukenya1, Sarah Bunoti1, Juliet Kiguli1
1Makerere University College of Health Sciences, School of Public Health, Department of Community Health and Behavioural Sciences, 2Centre of Excellence for Maternal, Newborn and Child Health, Makerere University School of Public Health, 3Makerere University College of Health Sciences, School of Public Health, Department of Health Policy Planning and Management
&Corresponding author
Lydia Kabwijamu, Makerere University College of Health Sciences, School of Public Health, Department of Health Policy Planning and Management. lkabwijamu@musph.ac.ug
Introduction:
The control of COVID-19 among children is mainly dependent on preventive strategies including proper use of facemask s, hand hygiene etiquette and social distancing. Despite ongoing risk communication, it is not clear how children understand COVID-19 and the control measures. We described children's understanding of COVID-19 transmission and the preventative strategies in Uganda.
Methods:
We conducted a cross-sectional study, between July and September 2020, among a random sample of 372 children (10 to 13 years) in Hoima district. We collected data using a structured questionnaire and observation checklists to elicit information on children's knowledge on COVID-19 transmission, its symptoms, preventive strategies and also their practices on handwashing and wearing a facemask. Descriptive analysis was conducted to summarize and describe children's knowledge and performance of COVID-19 preventive strategies.
Results:
Of the 372 participants, 94.35% were attending primary education. Overall, 75.40% knew that Coronavirus is spread through droplets; 85.21% knew at least one symptom, particularly cough (58.33%) and flu (58.06%); and 82.26% mentioned at-least four COVID-19 prevention measures unprompted. However, 2.15% correctly washed their hands as per the WHO 6-point handwashing standard. None followed all the WHO recommended steps when putting on a facemask and only 0.54% (2/372) followed the recommended steps when removing a facemask.
Conclusion:
Although most children were knowledgeable about COVID-19 transmission, signs and symptoms, and the preventive measures, a few could correctly demonstrate how to wash hands and how to wear or remove a facemask. Efforts for risk communication among children should focus on how they can perform Covid-19 preventive measures.
Introduction

The novel Coronavirus disease 2019 (COVID-19), continues to ravage lives around the world including children. Despite children appearing to have lower susceptibility to COVID-19 compared to the elderly, they can also be infected and can spread the virus to others [1]. Currently, available information shows that persons under 18 years have so far contributed about 1-5% of all the confirmed cases worldwide [2-4]. In Uganda, the number of COVID-19 cases continues to rise, with a cumulative number of 84,979 cases and 2,012 deaths that had been registered as of 8th July 2021 [5]. The number of cases among children in the country, which had initially had a gradual increase from 12 cases between March and June 2020 had exponentially increased to 92 cases by mid-September 2020.
Currently (by end of July 2021), a cumulative number of 1,383 cases below the age of 10 years and 3,384 cases between 10 and 19 years has been reported in the current ongoing second wave [
5,
6]. Besides the rising COVID-19 infections among children, other resulting impacts of the disease continue to significantly threatened many more children´s lives than the disease itself [
7]. During this period, children´s social lives have been drastically affected by the COVID-19 control measures that have restricted their movements, play and school [
8].
Current efforts to prevent COVID-19 are largely based on pharmaceautical measures such as vaccination and risk communication. However, among children, COVID-19 preventive measures are mainly non pharmaceutical and are greatly dependent on risk communication and correct practice of prevention strategies like hand washing, use of facemasks and maintaining social distance [
9,
10]. In Uganda, these measures are vividly promoted through continuous risk communication [
11]. However, this communication is mainly designed for adult audiences as opposed to both children and adults [
12].
In order to achieve effective management of COVID-19 in a country where over 50% of the population is below 18 years and majority residing in rural areas [
13], it was crucial to consider understanding children´s knowledge and practices regarding the COVID-19 prevention measures so that evidence-based strategies for strengthening and improving their safety and wellbeing are developed [
14]. Additionally, empowering children on how to overcome COVID-19 and enhancing their role as agents of change, is of national interest and is urgently required given its implications to reopening schools and intergenerational contacts [
15]. We therefore sought to describe children´s understanding of COVID-19 transmission and the preventative strategies to contribute to efforts of the ongoing COVID-19 risk-communication among children in Uganda. To the best of our knowledge, this is the first study to explore children´s understanding of COVID-19 and its prevention in Uganda.
Methods

Study setting
The study was conducted in Hoima Municipality located within Hoima District in Bunyoro sub-region, in western Uganda. The district is approximately 200 km by road from Kampala, the capital city of Uganda. Hoima Municipality has a population of approximately 122,700 people of which approximately 11.5% are children aged 10 to 13 years (13). The Municipality also hosts Hoima Regional Referral Hospital, the COVID-19 regional treatment Centre. Hoima Municipality was one of the areas in Uganda where the first cases of COVID-19 were reported. Additionally, Hoima District remains one of the high-risk districts for COVID-19 because it is among the border districts, which are more prone to receiving infected persons from neighboring countries through multiple porous border points. By the time of data collection, efforts to address the ongoing pandemic within the district were centered around COVID-19 risk communication, active disease surveillance and treatment of confirmed cases.
Study design and study population
We conducted a cross-sectional study using quantitative methods of data collection among children aged 10 to 13 years in Hoima Municipality. We focused on this age group because this category is usually left out in both children and adult surveys, but can also express themselves during data collection. In addition, apart from being at risk of COVID 19, children aged 10 to 13 years were more likely to be in upper primary level education and had had greater exposure to the COVID 19 messages unlike the younger ones. Besides, those aged 10 to 13 years were more likely to influence the practice of COVID-19 preventative practices unlike the younger ones. We included children who were aged 10 to 13 years irrespective of sex, who were residing within Hoima Municipality at the time of study. We excluded children aged 10 to 13 years who were resident within the selected vilages but were sick and thus unable to answer questions or those with severe disablitiy like the deaf or the blind who had no aids to correct the disability. We excluded them because we had no technical capacity nor the financial resources to enable them participate in the study. In particular we had no sign language interpreters nor braille typewriters to facilitate the discussions with children with the disabilities.
Sample size determination
We estimated a sample size of 385 using the Kish Leslie formula:

[
16] with the following parameters; 5% level of precision (δ), 1.96 standard normal deviation Z score corresponding to 95% confidence interval (Z). Since the actual proportion of children who understood or had knowledge of this phenomenon was not known, 50% was considered as the proportion, based on maximum variation [
17].
Sampling procedure
We used a multistage sampling approach. First, using simple random sampling, we sampled four wards, from the 16 that comprise Hoima Municipality. A list of villages per ward was generated by the Municipality authorities and each ward had at least nine villages. We then used simple random sampling to select four villages per ward, which gave us a cummulatve total of 16 sampled villages in the Municipality.
For each village, a sampling frame for all households with children between 10 and 13 years was developed by the village community heath worker, also called village health teams (VHTs) in Uganda. Each household on the village sampling frame was assigned a number starting from number one to the end without repetition. We then conducted simple random sampling with the help of a sampling application called research randomiser [
18] to generate a list of selected households from where to recruit the respondents. For each village, we cross checked that the sampling frame was continually numbered starting from number one to the end without repetition. We then entered the starting (one) and end number of the village sampling frame into the research randomiser Application and set it to generate a list of unsorted 24 unique numbers, without duplicates. The generated numbers represented the sampled households. At the household level, incase the selected household had more than one eligible child, the study team randomly selected one for interviewing.
Study variables and their measurement
Our key study variables included: 1) knowledge on COVID-19 transmission; 2) Knowledge on COVID-19 preventive measures; 3) handwashing practices and 4) how to wear or remove a non medical facemask. Knowledge on how COVID-19 is transmitted was a binary variable measured as yes or No. A child was considered knowledgeable if they answered that COVID-19 was transmitted through droplets of an infected person. Knowledge on COVID-19 preventive measures was measured using a likert scale. A child was given a point for each correct preventive measure mentioned unprompted. The cumulative points accrued by each child were used to categorise the children as either having no knowledge, fair/moderate knowledge or having good knowledge. A child was said to have no knowledge if they did not mention any correct preventive measure; fair or moderate knowledge if a child mentioned 1-3 correct preventive measures and good knowledge if a child mentioned 4 or more correct measures. Handwashing was categorized into proper handwashing if the observed child followed all the six steps of handwashing or no handwashing if the child missed or skipped one or more steps of handwashingg routine as defined by the World Health Organization. Likewise, for wearing and removing of non-medical facemasks, any child who wore or removed a facemask following all the WHO recommended steps for wearing and removing none medical facemask was categorized as having worn or removed the facemask correctly while those who missed a step or more were categorized as having not properly worn or removed a face facemask.
Data collection tools
Data was collected using an interviewer administered questionnaire and observation checklists that were previously pretested. These methods and tools have been used before among children to study various subjects and found effective [
19-22]. The questionnaire was developed based on the MOH multi-media messages on COVID-19, the WHO messages and Actions for COVID-19 Prevention and Control in Schools developed by UNICEF, WHO, ICRC in March 2020 [
23]. These messages were broadly being communicated across the nation through various media channels. The questionnaire also included a series of questions based on the Washington Group on Disability Statistics (WG) Short Set that are based on the framework of the World Health Organization´s International Classification of Functioning, Disability, and Health. These questions were included to assess the children´s self-reported difficulties and functionality for two core functional domains—seeing, and hearing. We focused on these two because the existing COVID-19 prevention messaging was majorly transmitted through visual and audio media at the time of data collection. We observed handwashing among all interviewed children using an observation checklist based on the WHO six steps for hand washing. To aid ease in comprehension, we adapted the “How to Wash Hands module in the “My Wash Handbook” produced in collaboration with UNICEF and Early Inspirations [
24]. This production was made for children and is pictorial. We conducted the observation after administering the child questionnaire. Observations of use of facemasks were conducted using the checklist for facemask use based on the World Health Organisation/ Ministry of Health´s Facemask s do´s and don´ts guidelines on how to wear and remove non surgical facemasks [
25]. The observation checklist and child questionnaire were designed in Open Data Kit (ODK) tool mounted onto android supported phones to facilitate electronic data capture.
Data collection processes
Our data collection processes were embedded in Child Centered Methodologies of research. Children were viewed as autonomous individuals with a voice and potential to express themselves. The research process focused on being fair and respectful to children [
26] and utilized data collection methods and practices congruent of the children´s developmental milestones [
27,
28]. Beyond the methodologies of data collection efforts were taken to reduce power imbalance and to conduct research in an ethical manner that protects children´s rights [
26,
29]. Data collection was conducted in homes, in an interactive conversational manner [
30] aided by the use of pictures and song/ play.
Hence, the data collection tools and processes were complemented by the use of pictures and intermittent breaks with song and/or a play. The ODK tool was formated with pictures illustrating various aspects associated with COVID-19, how it is spread, its symptoms or how to prevent it. The pictures also depicted use of facemasks and steps of hand washing. The study team moved with picture cards illustrating the the different aslects of COVID-19 as previously mentioned. In an instance where the children could not express themselves clearly, they were shown pictures and asked to point at a picture that depicted what they wanted to communicate. Play/ song was used as an ice breaker before the data collection started or as an intermittent break. A team of eight young (20 to 25 years) research assistants collected the data under the supervision of authors CNK, LK and AKT. The research assistants were trained for four days before data collection. Research assistants were trained on key research issues including interviewing skills, research ethics, data collection and management and child Centered methodologies of research. The training also covered aspects of COVID-19 with a focus on how it is spread; its signs and symptoms; how to prevent it or where and how to access help in case of a community suspected case.
Research assistants administered face-to-face interviews in privacy, in Runyoro the predominantly spoken local language in Hoima District. We used village health teams (VHTs) to gain community entry. At the household level, VHTs introduced the research assistants and their purpose of visit. The research assistants introduced the study objectives to the household head and also ensured that children understood the purpose of the research in which they were asked to participate. The research assistant then sought consent from the household head and assent from the child, prior to administering the interview and checklist. Cognizant of the COVID-19 risk, all research assistants and the respondents were required at all times to implement the COVID-19 prevention guidelines like wearing a facemask, keeping physical distance and hand sanitizing. No shaking of hands was allowed during data collection.
Data analysis
Since the purpose of this study was to describe the childrens´ understanding and practices on COVID-19 prevention strategies, we generated descriptive statistics for the different outcomes using STATA version 14. We present our findings with frequencies and their corresponding percentages.
Ethical considerations
We sought ethical approval from the Makerere University School of Public Health Higher Degrees Research and Ethics Committee (reference- protocol 835) and the Uganda National Council for Science and Technology (UNCST) (Reference number -HS830ES) prior to conducting the study. We also sought permission from Hoima District Local government before the study started. Informed consent and assent were obtained from each study participant. Given that the study was conducted during the COVID-19 pandemic, the study team worked closely with the Hoima district COVID-19 taskforce and upheld the COVID-19 control guidelines by the UNCST and Ugandan Ministry of Health. The study team was trained about COVID-19, how it is spread and how to prevent it. All participants in the study and the research team were provided with reuseable cloth facemasks and hand sanitizers. All study particpants and the research team were mandated to wear the facemasks at all times during the interviews. Likewise, hand hygiene was maintained and encouraged through use of hand sanitizer when paper and pen were to be used especially during the consent process. Interviews were conducted in the open while maintaining a safe distance of at least 6 feet. As, mandated by MOH Uganda and the UNCST, the study team members gave the family a talk about COVID-19 disease; how it is spread, its signs and symptoms and how it can be prevented.
Results
Demographic characteristics of participants
A total of 385 participants were initially identified and approached, 372 agreed to participate in the study. Hence a response rate of 96.62%. More than half, 55.91% (206/372) of the participants were female, about a quarter, 26.08% (97/372) were 13 years old and 27.42% (102/372) were 10 years old. Nearly all, 94.35% (351/372) were attending primary level education, and 3 (0.81%) were not enrolled for school. Eleven participants (2.96%) had some difficulties seeing, 2.96% (11/372) had difficulties hearing, and 21.29% (79/372) could not read at all
Table 1.
Knowledge on COVID-19; how it is spread and its signs and symptoms
Majority, 75.4% (279/372) of participants knew that the Coronavirus is spread through droplets.
Eighty-five percent of the participants knew at least one symptom of COVID-19. The symptoms known by most participants were: cough 58.33% (217/372); other flu like symptoms 58.06% (216/372) and fever 40.59% (151/372). Only three participants knew that sudden loss of smell or taste is a symptom of COVID-19.
Knowledge on COVID-19 disease preventive measures
Majority of participants, 82.26% (306/372) had moderate knowledge about COVID-19 prevention (mentioned 1-3 COVID-19 prevention measures unprompted). Seventeen percent (64/372) had good knowledge about the prevention of COVID-19 (mentioned 4 or more COVID-19 prevention measures unprompted). The most mentioned COVID-19 preventive measures were: “Frequent washing of hands with water and soap” by 81.99% (305/ 372), followed by “Always cover your nose and mouth with a facemask when outside the home” by 54.57 (203/372). On the other hand, none mentioned “Regularly clean frequently touched objects and surfaces” as a preventive measure
Table 2.
Observation of COVID-19 preventive practices
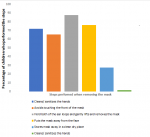
When putting on a facemask, none of the participants followed all the WHO recommended steps. However, twenty-two percent (83/372) washed their hands with water and soap before touching the facemask and 31.18% (116/372) avoided touching the facemask surface. Eight participants did not follow any of the recommended steps when putting on a face facemask
Figure 1.
On the other hand, when removing the face facemask, only two (0.54%) of the participants followed the recommended steps
Figure 2.
Hand washing practices among children aged 10 to 13 years in Hoima District
Only eight of the 372 participants (2.15%) practiced proper handwashing (followed all the six WHO steps for handwashing). The most performed steps were lathering and rubbing the hands with soap performed by 87.10% (324/372), followed by wetting the hands with water prior to lathering performed by 56.99% (212/372), followed by rubbing the nails tips on soapy palms performed by 47.85% (178/372) and washing of the wrist by 36.02% (134/372). Only 19.35% (72/372) and 11.56 (43/372) washed their thumbs and focused on rubbing the back of their hands and in between fingers respectively
Table 3.
Discussion
In this study, we sought to describe children´s understanding of COVID-19 spread, its preventive measures and practice. A considerable number of children knew that COVID-19 is spread through droplets. This could be a result of the continuous risk communication by the Ugandan government in the early stages of the outbreak in Uganda [31]. Studies have shown that children are likely to grasp repetitive information [32, 33], which could have contributed to their knowledge on COVID-19 symptoms often communicated.
Additionally, majority of the children mentioned at least one COVID-19 symptom, especially, coughing and flu like symptoms. Children could have easily understood these symptoms, such as cough and flu, since they are common disease symptoms in Uganda where infectious diseases are highly prevalent. Similarly, a study among primary school going children (8 to 15 years) in Uganda also found that children were able to recognize symptoms such as high body temperature, headache, diarrhea, weakness, and appetite loss to tell that they were sick [
34]. Easy identification of COVID-19 symptoms by children can also be attributed to the fact that most African children are mostly affected by infectious diseases, which present with some symptoms similar to those with COVID-19. Besides, African children are hospitalized with influenza and have influenza-associated hospitalization rates more than three times higher than those of children in industrialized countries [
35]. However, few children knew that a person with COVID-19 can be asymptomatic. This could also be because the initial risk communication in the country, focused on overt signs and symptom like fever and cough.
Knowledge of the COVID-19 preventive strategies was moderate among the children. Majority could mention at least one preventative strategy for COVID-19. This could be attributed to the overwhelming efforts in place to articulate the COVID-19 preventative strategies. Within the area, the media, and conversations within the community were focused on COVID-19 prevention. Additionally, this knowledge could be attributed to the fact that the population had heightened anxiety and fear of COVID-19 for a number of reasons for instance 1) apart from COVID-19 being an emerging disease, it´s countrywide preventative measures which brought everything to a standstill were scary enough for people to pay attention to messages of its prevention irrespective of age. In addition, the fact that Hoima Municipality reported a case within a month of COVID 19 introduction to Uganda could have contributed to anxiety and fears that forced the people to attentively listen and pay attention to messages of its prevention irrespective of age. This fear could have influenced the populations efforts to self protect thus increasing attention to the disseminated preventative startegies irrespective of age. From the findings, majority of the households had access to radio which was one the major sources of COVID-19 prevention messages. We hypothesize that since children were out of school and non essential movements restricted, they had ample time to access media information about self protection.
Despite the fact that children knew the protective importance of wearing a facemask, minority demonstrated how to correctly put on and remove a facemask as recommended. The low competence of wearing facemasks could be because coveeing the nose and mouth using a facemask is a new phenomenon and expected behavior could take time for many to implement. Studies have shown that attainment and maintenance of new health behaviours takes time and is often difficult to implement [
36,
37]. However, this could be an indicator that there is a gap in the risk communication: while messages broadcasted in the country try to demonstrate how a facemask is utilized, the information broadcasted probably mainly fits adult consumption and interpretation leaving out the children. Though the study did not capture information from children with disability, the findings point to the need to also broadcast information that is for children with difficulties in seeing and hearing.
Besides, poor adherence to and satisfaction with COVID-19 preventive measures among adults in Uganda has been reported (31). It is also not known whether adults are able to follow the recommended steps for wearing a facemask. Since children learn well through observation, lack of appropriate modeling by adults due to either adults´ inability to use a facemask as recommended or their poor compliance to use a facemask could consequently be affecting children´s practice in facemask usage [
38].
Moreover, a majority of children in this study demonstrated poor hand washing practice even though they mentioned that it was an important preventive measure. One of the reasons for poor handwashing practice could be that many people habitually wash their hands but incorrectly, even among health workers [
39]. A recent study among adults in Uganda also found out that about 80% of the participants could not complete all the WHO recommended steps of handwashing. However, participants that had been taught handwashing were more likely to have better hand hygiene knowledge and practice [
40]. This could also be an indicator that risk communication about handwashing lacks an element of “how” handwashing should be done or if not, it is not portrayed in a way that the public (both adults and children) can comprehend. Therefore, hand hygiene health education needs to further be scaled to include sensitization on how handwashing should be done.
However, this study should be regarded within the context of some limitations. The study was conducted at a time when children were at home and had not returned to school. Therefore, certain facets of their understanding of COVID-19 might be affected when they resume schooling. Nonetheless, our study shows that the gap is not in the knowledge about COVID-19 but in the practice of the different preventive measures. Also, our study being cross sectional in desgn and with a descriptive analysis approach may not depict causal effect or relationships, but its strength is in the rich elaboration of the knowledge and deficiencies in the practices of COVID-19 prevention measures among this population, which was the aim of the study. Lastly we did not capture data from children with hearing and visual disabilities. This could have created selection bias.
Conclusion
We found that most children were knowledgeable about how COVID-19 is spread and knew several COVID-19 signs and symptoms. Most children knew the preventive measures communicated but they were not competent enough to demonstrate how these measures are being practiced especially handwashing and how to use a facemask.
Recommendations
We recommend that efforts of risk communication for this age group should focus more on how to practice the recommended practices. This could be achieved through simplified step-by-step communication of the procedures or through more visual communication media while catering for children with visual and hearing disabilities.
What is known about this topic
- COVID-19 affects all irrespective of age
- COVID-19 prevention among children below 18 years largely depends on the correct and consistent implementation of the preventive measures such as frequent had washing, proper use of facefacemask s and maintaining social distance.
What this study adds
- This work contributes to understanding how the COVID-19 preventive are practiced among the children
- The research highlights a knowledge to practice gap of the COVID-19 preventive measures in this age group and the imperative need to improve the communication strategies around how to implement the preventive measures for this age group.
Competing interests
The Authors declare no competeing interests
Authors' contributions
CNK contrubuted to the conceptualisation of the study, preparation of the study protocol, training of research assistants, supervision of data collection, analysis and manuscript writing. LK contributed to the conceptualisation of the study, preparation of the study protocol, training of research assistants, supervision of data collection, analysis and manuscript writing. MN contributed to the conceptualisation of the study, preparation of the study protocol, data analysis and manuscript writing. AT contrubuted to the preparation of the study protocol, training of research assistants, supervision of data collection, analysis and manuscript writing. JB contrubuted to the preparation of the study protocol, training of research assistants, supervision of data collection, analysis and manuscript writing. SB contrubuted to the preparation of the study protocol, training of research assistants, supervision of data collection, analysis and manuscript writing. JK contrubuted preparation of the study protocol, training of research assistants, supervision of data collection, analysis and manuscript writing
Tables and figures
Table 1: Demographic characteristics of participants
Table 2: Description of Covid-19 preventive measures known among children aged 10 to 13 years in Hoima district
Table 3: Observation of hand washing among children aged 10 to 13 years in Hoima district
Figure 1: Percentage of children who performed the recommended steps when wearing a face mask
Figure 2: Percentage of children who performed the recommended steps when removing a face mask
References
- Evliyaoğlu O, Kılınç AA, Önal P, Aygün F, Çokuğraş H. COVID-19 in children. Turk Pediatri Ars. 2020 Jun 19;55(2):85.https://doi.org/10.14744/turkpediatriars.2020.07742 PubMed | Google Scholar
- Tagarro A, Epalza C, Santos M, Sanz-Santaeufemia FJ, Otheo E, Moraleda C, Calvo C. Screening and Severity of Coronavirus Disease 2019 (COVID-19) in Children in Madrid, Spain. JAMA Pediatr. 2020 Apr 8:e201346.https://doi.org/10.1001/jamapediatrics.2020.1346 PubMed | Google Scholar
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. Jama. 2020;323(13):1239-42.https://doi.org/10.1001/jama.2020.2648 Google Scholar
- Ranabothu S, Onteddu S, Nalleballe K, Dandu V, Veerapaneni K, Veerapandiyan A. Spectrum of COVID-19 in children. Acta Paediatr. 2020 Sep;109(9):1899-1900.https://doi.org/10.1111/apa.15412 PubMed | Google Scholar
- MOH, Uganda. Covid-19 Status in Uganda. 2020. Uganda: MOH. Accessed May 2020.
- Government of Uganda (GoU). COVID-19 Response Information Hub. Government of Uganda. 2021. Accessed July 2021.
- World Vision. COVID-19: Children face the highest risk. World Vision. 2020. Accessed May 2020.
- Save the Children. Keeping children learning and safe during Covid-19. Save the Children. 2020. Accessed May 2020.
- Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924.https://doi.org/10.1016/j.ijantimicag.2020.105924 PubMed | Google Scholar
- Khosravi M. Perceived risk of COVID-19 pandemic: the role of public worry and trust. Electronic Journal of General Medicine. 2020; 4(17): 1-2.https://doi.org/10.29333/ejgm/7856 Google Scholar
- Sun P, Lu X, Xu C, Sun W, Pan B. Understanding of COVID-19 based on current evidence. J Med Virol. 2020 Jun; 92(6):548-551. https://doi.org/10.1002/jmv.25722 PubMed | Google Scholar
- Soma GJ. Communicating to children about the COVID-19 pandemic. South Sudan Medical Journal. 2020 Jul 9; 13(2):60-3. Google Scholar
- UBOS and Rockville M, USA. The national population and housing census 2014 - main report, Kampala, Uganda. UBOS. 2016. AccessedSept 2022.
- Uganda National Population Council. State of Uganda population report 2018. Uganda National Population Council. 2018. Accessed Sept 2022.
- Li X, Xu W, Dozier M, He Y, Kirolos A, Lang Z, Song P, Theodoratou E; UNCOVER. The role of children in the transmission of SARS-CoV2: updated rapid review. J Glob Health. 2020 Dec;10(2):021101.https://doi.org/10.7189/jogh.10.021101 PubMed | Google Scholar
- Kish L. Survey sampling. 1965. New York: Wiley Pty Ltd. 1985. Google Scholar
- Singh A, Masuku M. Sampling ttechniques & determination of sample size in applied statistics research: an overview. IjecmCoUk. 2014; 2(11): 1-22. Google Scholar
- Urbaniak GC, & Plous, S. Research randomizer Version 4.0 ed2013 p Computer Software.
- Christian BJ, Pearce PF, Roberson AJ, Rothwell E. It's a small, small sorld: data collection strategies for research with children and adolescents. Journal of Pediatric Nursing. 2010; 25(3):202-14.https://doi.org/10.1016/j.pedn.2009.01.003 . Google Scholar
- 1. Elyazgi M.Review of gathering data instruments and methods in children research . IJET [Internet]. 2018 Aug 8 [cited 2022 Sep 16];7(3.21):311. http://dx.doi.org/10.14419/ijet.v7i3.21.17179
Google Scholar
- Flanagan SM, Greenfield S, Coad J, Neilson S. An exploration of the data collection methods utilised with children, teenagers and young people (CTYPs). BMC Res Notes. 2015 Mar 1; 8:61.https://doi.org/10.1186/s13104-015-1018-y PubMed | Google Scholar
- Morgan M, Gibbs S, Maxwell K, Britten N. Hearing children's voices: methodological issues in conducting focus groups with children aged 7-11 years. Qualitative Research. 2002;2:5-20.https://doi.org/10.1177/1468794102002001636 Google Scholar
- UNICEF. Key messages and actions for COVID-19 prevention and control in schools. UNICEF. 2020. Accessed Sept 2022.
- WHO. Wash workbook. WHO. 2020. Accessed Sept 2022.
- WHO. Coronavirus disease (COVID-19) advice for the public: When and how to use masks. 2020. Accessed Aug 2020.
- Graham A, Powell MA, Anderson D, Fitzgerald R, Taylor NJ. Ethical research involving children. Florence: UNICEF Office of Research-Innocenti; 2013 Mar 31.
- Gibson JE. Interviews and focus groups with children: Methods that match children's developing competencies. Journal of Family Theory & Review. 2012; 4(2):148-59. Google Scholar
- Punch S. Research with children: the same or different from research with adults? Childhood. 2002; 9(3):321-41. Google Scholar
- Nairn A, Clarke B. Researching children: Are we getting it right?: A discussion of ethics. International Journal of Market Research. 2012; 54(2):177-98. Google Scholar
- Mondada L. The conversation analytic approach to data collection. The handbook of conversation analysis. 2013:32-56. Google Scholar
- Amodan BO, Bulage L, Katana E, Ario AR, Fodjo JNS, Colebunders R, Wanyenze RK. Level and Determinants of Adherence to COVID-19 Preventive Measures in the First Stage of the Outbreak in Uganda. International journal of environmental research and public health. 2020; 17(23):8810. https://doi.org/10.3390/ijerph17238810 PubMed | Google Scholar
- Committee on the Science of Children Birth to Age 8: Deepening and Broadening the Foundation for Success; Board on Children, Youth, and Families; Institute of Medicine; National Research Council; Allen LR, Kelly BB, editors. Transforming the Workforce for Children Birth Through Age 8: A Unifying Foundation. Washington (DC): National Academies Press (US); 2015. Google Scholar
- Darling-Hammond L, Flook L, Cook-Harvey C, Barron B, Osher D. Implications for educational practice of the science of learning and development. Applied Developmental Science. 2020;24(2):97-140.https://doi.org/10.1080/10888691.2018.1537791 . Google Scholar
- Akello G, Reis R, Ovuga E, Rwabukwali CB, Kabonesa C, Richters A. Primary school children's perspectives on common diseases and medicines used: implications for school healthcare programmes and priority setting in Uganda. Afr Health Sci. 2007 Jun; 7(2):73-9.https://doi.org/10.5555/afhs.2007.7.2.73 PubMed | Google Scholar
- Lafond KE, Nair H, Rasooly MH, Valente F, Booy R, Rahman M, Kitsutani P, Yu H, Guzman G, Coulibaly D, Armero J, Jima D, Howie SRC, Ampofo W, Mena R, Chadha M, Sampurno OD, Emukule GO, Nurmatov Z, Corwin A, Heraud JM, Noyola DE, Cojocaru R, Nymadawa P, Barakat A, Adedeji A, von Horoch M, Olveda R, Nyatanyi T, Venter M, Mmbaga V, Chittaganpitch M, Nguyen TH, Theo A, Whaley M, Azziz-Baumgartner E, Bresee J, Campbell H, Widdowson MA, Global Respiratory Hospitalizations—Influenza Proportion Positive (GRIPP) Working Group. Global role and burden of influenza in pediatric respiratory hospitalizations, 1982-2012: a systematic analysis. PLoS medicine. 2016; 13(3):e1001977.https://doi.org/10.1371/journal.pmed.1001977 PubMed | Google Scholar
- Kwasnicka D, Dombrowski SU, White M, Sniehotta F. Theoretical explanations for maintenance of behaviour change: a systematic review of behaviour theories. Health psychology review. 2016; 10(3):277-96.https://doi.org/10.1080/17437199.2016.1151372 PubMed | Google Scholar
- Gardner B, Lally P, Wardle J. Making health habitual: the psychology of ‘habit-formation’and general practice. British Journal of General Practice. 2012;62(605):664-6.https://doi.org/10.3399/bjgp12X659466 PubMed | Google Scholar
- Gaskins S, Paradise R. Chapter five learning through observation in daily life. The anthropology of learning in childhood. 2010; 85:85-110. Google Scholar
- Jemal S. Knowledge and Practices of Hand Washing among Health Professionals in Dubti Referral Hospital, Dubti, Afar, Northeast Ethiopia. Adv Prev Med. 2018 Nov 22;2018:5290797.https://doi.org/10.1155/2018/5290797 PubMed | Google Scholar
- Nuwagaba J, Ashok DD, Balizzakiwa T, Kisengula I, Nagaddya EJ, Rutayisire M. The era of coronavirus; knowledge, attitude, practices, and barriers to hand hygiene among Makerere University students and Katanga community. Risk Manag Healthc Policy. 2021 Aug 14; 14:3349-3356.https://doi.org/10.2147/rmhp.s318482 PubMed | Google Scholar