A descriptive study of all COVID- 19 clients in Copperbelt province, Zambia 2020: A retrospective analysis
Lwito Salifya Mutale1,2,&, Olufemi Olamide Ajumobi3,4, Francis Nanzaluka2, Justine Chileshe5, Patrick Sakubita6, Nyambe Sinyange6, Paul Msanzya Zulu6, Muzala Kapina6, Nathan Kapata6, Christopher Dube2, Gorge Chansa Mukupa2, Golden Kangala2, Albert Mweembe2, Justor Banda2, Charles Sakulanda2, James Nonde2, Robert Zulu2, Victor Mukonka6, David Kasanga Mwakazanga5, Gershom Chongwe5
1Zambia Field Epidemiology Training Programme, Lusaka Zambia, 2Ministry of Health, Zambia, 3School of Public Health, University of Nevada, Reno, Nevada, United States of America, 4Nigeria Field Epidemiology and Laboratory Training Program, Abuja, Nigeria, 5Tropical Disease Research Centre, Zambia, 6Zambia National Public Health Institute, Lusaka, Zambia
&Corresponding author
Lwito Salifya Mutale, Ministry of health, Kitwe, Zambia. lwitosalifyanji@gmail.com
Introduction:
Zambia is among the countries affected by the COVID-19 pandemic. This study describes the socio-demographic characteristic of the population affected, survival from infections, and identifies health-related factors associated with COVID-19 infections in the Copperbelt province of Zambia.
Methods:
We analyzed COVID-19 related data on clients tested from 19th February, 2020 to 8th July, 2020 The data comprised laboratory test data where a positive COVID-19 infection was confirmed with RT-PCR, and data on a person's socio-demographic characteristics, symptoms, and co-morbidities, collected using a structured questionnaire administered to consenting persons during testing. In addition, we reviewed patient medical files for hospitalised individuals.
Results:
7650 of 8644 tested clients were included in the analysis. The median age of all the patients was 32 years (range: 1 month to 95 years). The majority (64.4%) were males and the largest number (25.7%) of patients was from the Ndola district. The positivity rate among all the tested clients was 6.2% (n=475). Case fatality rate (CFR) among the hospitalised patients was 18.8%. Age was not significantly associated with mortality (p = 0.338).
Conclusion:
Despite a rather low positivity rate, mortality among hospitalized patients was very high. All ages infected with the virus had the same likelihood of dying. There is a need to investigate the cause of the high mortality among hospitalised patients.
Introduction

The World Health Organization (WHO) declared the Coronavirus disease 2019 (COVID-19) outbreak pandemic on March 11, 2020 [1]. This outbreak has claimed over 1,400,000 lives worldwide [2]. In Africa, COVID- 19 has affected almost all the countries with a total of 874,036 confirmed cases and 18,498 deaths as of 25th November, 2020 [3].
In Zambia, the outbreak has affected all the 10provinces, with a total of 17, 730 cases and 357 deaths as of 5th November 2020 (CFR 2.0%) [
3]. Earlier in the outbreak, after mass screening in Nakonde, a border town with Tanzania, results were found to comprise 80% of the overall cases in the country [
4]. This led to mass screening in other provinces with major border towns by the Ministry of Health (MOH), Zambia to understand the disease burden. Furthermore, like other governments around the world, the Zambian government put up measures to mitigate the further spread of the disease [
5-9]. Among the preventive measures, a policy to hospitalise all positive patients as a means of isolation to reduce further spread was put in place. However, despite all the measures put up to avert the pandemic, confirmed COVID- 19 cases and deaths continued to increase in the Copperbelt province.
A greater need for more targeted preventive measures was essential to preventing new cases. Therefore, data on epidemiological and clinical characteristics was needed to provide evidence-based recommendations on preventive measures. We performed a formal analysis of data to determine the positivity rate of COVID-19 disease in the Copperbelt province, describe the populations affected and identify risk factors, to inform the preventive and control measures to avert new cases.
Methods

Study design and population
This study entailed secondary analysis of data on COVID-19 tested clients collected from 19th February 2020 to 08th July, 2020, in the Copperbelt province of Zambia. The Copperbelt province had a population of 2,675,446 in 2010/2019 (CSO projections). The province is Zambia´s second largest population centre and is home to most of the mining activities for the country. The study population comprised of all individuals tested for COVID-19 in Copperbelt Province and were line-listed in the event-based surveillance system.
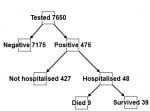
COVID-19 was confirmed by detection through reverse transcriptase polymerase chain reaction (RT?PCR) from a respiratory tract specimen using a DaAn kit (DaAn Gene Co, China). These tests were performed at the Tropical Disease Research Centre (TDRC) laboratory. Positive clients were persons with laboratory confirmation of COVID-19 infection and negative clients were persons with laboratory confirmation of not having COVID-19 infection. A total of 7,650 individuals were included in the analysis, of whom 7,175 were found negative, and 475 were positive. Of the 475 positive patients, 48 were held in isolation facilities and nine of the isolated patients died
Figure 1
Data collection and processing
As part of mass testing, trained disease surveillance personnel from the Zambian MOH administered a structured questionnaire from each consenting individual to collect data on socio-demographic, symptoms, co-morbidities, medications, and treatment outcome. The questionnaires were adapted from the WHO COVID-19 surveillance forms (case investigation form (Form C), contact tracing form (Form D) and monitoring form (Form E). Data were then entered using excel to form the provincial line list of all the COVID- 19 clients. Additionally, samples (nasopharyngeal or oral-pharyngeal) from the consenting individuals were collected and transported to designated laboratories for testing.
The questionnaires were entered into a Microsoft
® Excel worksheet on password protected computers in a restricted access office at provincial administration level. Each questionnaire was entered in two separate worksheets by different data entry clerks, resulting in two separate databases of the same questionnaires. The double data entry was to facilitate data validation. Entries in the two resulting databases were compared using the statistical software SAS 9.4, for mismatched and missing values as part of the data validation process. Mismatches and missing values were resolved with reference to the structured questionnaire entries and client laboratory records.
In addition to the data extracted from the line list, we reviewed patient medical files for the isolated individuals. We extracted data on exposure, history of travel, demographics, signs and symptoms on swabbing, co-morbidity, laboratory results, co-infection with other respiratory pathogens, treatment given and clinical outcomes, using Epi Info 7 software within-built validity and consistency checks for entries. The resulting database was then exported into the SAS 9.4 for cleaning and statistical analyses.
Data analysis
Categorical variables were described using frequencies and percentages, while means and standard deviations were used to describe continuous variables. Statistical significance for differences between independent samples was assessed using the two-sample T-test for normally distributed continuous variables, and the Wilcoxon rank-sum test for non-normally distributed continuous variables. The Shapiro-Wilk´s test was used to assess normality in the distribution of continuous variables. For descriptive analysis, test outcome status (positive or negative) was treated as the dependent variable. Clinical, socio-demographic, and geographical factors were treated as independent variables. Fisher´s exact test was used to assess significance of associations and results were presented as statistically significant at p-value <0.05.
Ethical considerations
Ethical approval was obtained from the University of Zambia Biomedical Research Ethics Committee (IRB. Number. 1124-2020) and the National Research Authority. Only de-identified data were analyzed. Data were stored on password protected computers by the Provincial Health Office, Ministry of Health and Zambia National Public Health Institute.
Results
As of 8 June 2020, 8644 clients were tested for COVID-19 infection from the Copperbelt province, of which 7650 were included in the analysis after cleaning. The median age of participants was 32 years (range: 1 month to 95 years). A quarter (25.3%, n=1849) of the participants were aged 20 to 29 years old, and a few (0.3%, n=21) were below 1 year old. Majority were males (60.4%, n=4607). Ndola district, with 1966 had the largest number of participants, accounting for 25.7% of all samples in the province and the least was Luanshya district accounting for only 60 participants (0.8%). The positivity rate among all the tested clients was 6.2% (n=475) Table 1 with a CFR of 1.7% (n=9) (Not shown).
Among the tested clients, age was slightly higher for positive clients than for negative clients. Mean age was 35.7 (standard deviation =±15.1 years) for positive clients and mean age was 33.1 (standard deviation =±14.9 years) for negative clients. Median age among positive clients was 34 years (ranged: 2 months to 85 years old). Most of the positive cases were from Kitwe district (41.9%, 199/475), followed by Chililabombwe district (23.8%, 113/475), Chingola district (14.7%, 70/475), Ndola district (10.7%, 51/475) and Mufulira district (5.9%, 28/475)
Table 1.
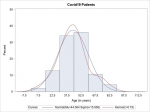
Overall, 48 of the 475 positive patients were admitted to a dedicated isolation health facility for COVID-19 patients. Among the admitted 48, 9 died (CFR after hospitalization = 18.8%). Among the patients who were hospitalised, age distribution between survivors and non-survivors was normally distributed
Figure 2. Majority of the hospitalised patients were truck drivers (42.5%, n=17), followed by those in self-employment (12.0%, n=5). All of the patients who died were aged 30 or above, with most (44.4%, 4/9) aged 60 or above.
Demographic characteristics of all admitted patients with COVID- 19 according to outcome are shown in
Table 2. Among the hospitalised patients, age was higher for non-surviving patients than for surviving patients. Mean age was 58.3 (standard deviation =± 16.3 years) for non-surviving patients and mean age was 40.7 (standard deviation =± 14.1 years) for surviving patients. Of the hospitalised patients, majority were males (72.9%). And most (42.5) of the hospitalised patients were truck drivers (42.5%), followed by those in self-employment (12.5%). There were slightly more (55.6%, 5/9) males than females among the patients that died.
A total of 48 files for hospitalised patients were reviewed from three dedicated COVID-19 isolation facilities in the province. Symptoms, co-morbidities, and medications of all hospitalised patients with COVID- 19 from patient files in Copperbelt province are shown in
Table 3. Only 8.3% (4/48) of the admitted patients were ventilated, and only 1 of the patients that were ventilated survived. Less than half (45.8%, 22/48) presented with symptoms at admission, and all the patients who died presented with symptom at admission. Fever/chills, coughing and shortness of breath were the symptoms the patients who died mostly (44.4%, 4/9) presented with at admission. This was followed by diarrhoea, nausea/vomiting and headaches (22.2%, 2/9). At 55.6% (5/9), cardiovascular disease was the leading co-morbidity/chronic medical illness among the patients who died, and this finding was significantly associated with mortality (P = 0.012). Further, our results show that HIV infection was not significantly associated with mortality (P = 0.601).
Survival of hospitalised COVID-19 patients by medications/therapy administered was disaggregated by presence of co-morbidities in
Table 4. Among patients with co-morbidities, the proportion of patients who were treated with either azithromycin or vitamin c or both, and survived was significantly higher (93.3% and 53.3% respectively) (P = <0.001 and P = 0.019 respectively), compared to those who were not treated with azithromycin and/or vitamin c.
Discussion
This analysis describes the socio-demographic characteristic of the population affected, identifies health related factors associated with COVID-19 infections and further describes survival from infections on the Copperbelt province in Zambia. The positivity rate among all the tested clients was 6.2% by 8th June, 2020 in the province. Our analysis found CFR of approximately 1.7% among all the tested clients and 18.8% among the hospitalized patients. Our findings on CFR (1.7%) were lower than those found in similar studies conducted around the world [10-12]. However, this conclusion might be premature since the province may not have reached the peak of the pandemic at that time of the study.
Our results are consistent with findings from a study by Nachega (2020) that have shown a higher number of males testing positive compared to females [
5], however, these results were not statistically significant. Furthermore, our study contradicts findings from studies that have been carried out elsewhere [
6,
10] which reported that children were at a lower risk of becoming infected.
Presence of symptoms was significantly higher among non-surviving hospitalized patients (100%) than among the surviving hospitalized patients (33%).Consistent with the majority of the studies conducted around the globe, our results showed that diarrhoea, abdominal pain, fever, cough, fatigue, headache, haemoptysis, dyspnoea, lymphopenia, dry cough and myalgia were the most commonly reported symptoms at onset of COVID-19 [
6-9,13-15]. Among the hospitalised patients, only general weakness, shortness of breath, nausea and vomiting of the symptoms reported were significantly associated with mortality.
Of the five types of co-morbidities that were reported by the hospitalized patients, only cardiovascular disease was found to be significantly associated with mortality. However, it is important to note that majority (78%) of the patients with fatal outcomes had a co-morbidity, consistent with other studies done around the world [
5,
16,
17]. With sub-Saharan Africa accounting for two thirds of the global human immunodeficiency virus (HIV) burden, and Zambia not being excluded, concerns of possible experiences of high burden of COVID-19 disease with critical outcomes where expressed in the earlier stages of the pandemic [
5,
18-20]. With a growing body of literature which indicates persons living with HIV are at greater risk of severe disease and critical outcomes [
21,
22]. In our study, only two of the nine patients with HIV infection had a fatal outcome. This finding could be attributed to the fact that the patient´s immune systems were not compromised since all HIV positive+ patients who survived were on anti-retroviral therapy treatment (ART) [
23-25]. However, our finding of lack of association between HIV and severe COVID- 19 outcome could have been because of the small sample size.
Furthermore, although the illness has been found to be more fatal among those older than 60 years old, especially with co-morbidities, our results show that patients aged less than 60 years old with similar co-morbidities were also at very high risk of fatal outcomes due to COVID-19. Both patients who had HIV infection and died were below the age of 60 (40 and 53 years).
Our study was not without limitations. The line list used had some omissions and errors with regards to recordings on age, sex and date of disease onset that made it difficult at analysis. Although all the patient files were available, another limitation was that some patient´s charts were either incomplete or had some missing pages, making it impossible to collect certain information on some variables mentioned in literature such as medication, co-morbidities, and travel history. Lastly, the sample size of hospitalised patients was small making it impossible for us to run regression analysis, hence limiting our ability to draw inferences.
Conclusion
In conclusion, our analysis has demonstrated that the patients with COVID-19 disease on the Copperbelt province of Zambia had a risk factor profile that was similar to many other populations. This study has shown that there was a high CFR among hospitalised patients in the Copperbelt Province of Zambia. There is need for improvement in case management to improve outcomes in this population.
What is known about this topic
- Coronavirus disease 2019 (COVID-19) has affected majority of countries worldwide which has economic and social challenges and different countries have put up measures to curb further transmission;
- Most commonly reported symptoms around the globe were diarrhoea, abdominal pain, fever, cough, fatigue, headache, myalgia, loss of appetite, irritability, confusion, general body weakness, nausea, vomiting, shortness of breath, sore throat and chills;
- COVID-19 illness was found to be more fatal among those older than 60 years old and more especially with co-morbidities.
What this study adds
- Provides estimates of the positivity rate of COVID-19 and the description of all clients in Copperbelt province;
- COVID-19 has affected all the age groups on the Copperbelt province including children;
- High CFR among hospitalised patients in the Copperbelt Province of Zambia could be due to inadequate case management methods as the disease is still evolving.
Competing interests
Authors declare no competing interests.
Authors' contributions
LSM, GC, FN, NS, NK, MK, and JC conceived and designed the study. PS, PNZ, GM, AM and GK contributed to data preparation. LSM and DKM performed data analysis and writing of the manuscript. OOA, GC, CD, JB, VM, RZ, JN and CS guided the analysis and interpretation of data, and critically revised the manuscript. All authors read and approved the final draft of the manuscript.
Acknowledgments
We would like to express gratitude to Ministry of Health and TDRC for affording us access to the data for the study, without which this paper would not have been possible. Staff at the isolation facilities on the Copperbelt with whom some of the data was extracted deserve appreciation for support given during the whole process of working on this study.
Tables and figures
Table 1: Demographic characteristics of 7650 COVID- 19 tested clients, by test outcome (to June 8, 2020)
Table 2: Demographics characteristics of all hospitalized patients with COVID- 19 (to June 8, 2020)
Table 3: Symptoms, co-morbidities, and medications of all hospitalized patients with COVID- 19, in Copperbelt province (to June 8, 2020)
Table 4: Survival of hospitalized COVID- 19 patients by medications/ therapy administered disaggregated by presence of co-morbidities
Figure 1: Data flow for the patients included in this study
Figure 2: Ages of all hospitalised patients with Covid- 19
References
- Eurosurveillance Editorial Team. Note from the editors: World Health Organization declares novel coronavirus (2019-nCoV) sixth public health emergency of international concern. Eurosurveillance. 2020 Feb 6; 25(5):200131e. Google Scholar
- WHO. Coronavirus Disease (COVID-19) Dashboard. WHO. Accessed Jul 2020.
- AfricaNews. Africa COVID-19 stats: 594,955 cases; 13,246 deaths; 295,242 recoveries. Africanews. 2020. Accessed Jul 2020.
- Anadolu Agency (AA). COVID-19: Zambia, Tanzania in talks over border closure. Anadolu Agency. 2020. Accessed Jul 2020.
- Nachega J, Seydi M, Zumla A. The Late Arrival of Coronavirus Disease 2019 (COVID-19) in Africa: Mitigating Pan-continental Spread. Clin Infect Dis. 2020 Jul 28;71(15):875-878.https://doi.org/10.1093/cid/ciaa353 PubMed | Google Scholar
- Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, Wang M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA. 2020 Apr 14;323(14):1406-1407.https://doi.org/10.1001/jama.2020.2565 PubMed | Google Scholar
- Calisher C, Carroll D, Colwell R, Corley RB, Daszak P, Drosten C, Enjuanes L, Farrar J, Field H, Golding J, Gorbalenya A, Haagmans B, Hughes JM, Karesh WB, Keusch GT, Lam SK, Lubroth J, Mackenzie JS, Madoff L, Mazet J, Palese P, Perlman S, Poon L, Roizman B, Saif L, Subbarao K, Turner M. Statement in support of the scientists, public health professionals, and medical professionals of China combatting COVID-19. The Lancet. 2020 Mar 7;395(10226):e42-3.https://doi.org/10.1016/S0140-6736(20)30418-9 . Google Scholar
- Jin X, Lian JS, Hu JH, Gao J, Zheng L, Zhang YM, Hao SR, Jia HY, Cai H, Zhang XL, Yu GD, Xu KJ, Wang XY, Gu JQ, Zhang SY, Ye CY, Jin CL, Lu YF, Yu X, Yu XP, Huang JR, Xu KL, Ni Q, Yu CB, Zhu B, Li YT, Liu J, Zhao H, Zhang X, Yu L, Guo YZ, Su JW, Tao JJ, Lang GJ, Wu XX, Wu WR, Qv TT, Xiang DR, Yi P, Shi D, Chen Y, Ren Y, Qiu YQ, Li LJ, Sheng J, Yang Y. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut. 2020 Jun;69(6):1002-1009.https://doi.org/10.1136/gutjnl-2020-320926 PubMed | Google Scholar
- Pan L, Mu M, Yang P, Sun Y, Wang R, Yan J, Li P, Hu B, Wang J, Hu C, Jin Y, Niu X, Ping R, Du Y, Li T, Xu G, Hu Q, Tu L. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am J Gastroenterol. 2020 May;115(5):766-773. https://doi.org/10.14309/ajg.0000000000000620 PubMed | Google Scholar
- Velavan TP, Meyer CG. The COVID-19 epidemic. Trop Med Int Health. 2020 Mar;25(3):278-280.https://doi.org/10.1111/tmi.13383 PubMed | Google Scholar
- Bassetti M, Vena A, Giacobbe DR. The novel Chinese coronavirus (2019-nCoV) infections: Challenges for fighting the storm. Eur J Clin Invest. 2020 Mar;50(3):e13209.https://doi.org/10.1111/eci.13209 PubMed | Google Scholar
- Y Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, Wu Y, Zhang L, Yu Z, Fang M, Yu T, Wang Y, Pan S, Zou X, Yuan S, Shang Y. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020 May;8(5):475-481. https://doi.org/10.1016/s2213-2600(20)30079-5 PubMed | Google Scholar
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020 May;109:102433.https://doi.org/10.1016/j.jaut.2020.102433 PubMed | Google Scholar
- Umavathi S, Subash M, Thiruvarasan K, Punithavalli S, Manikandan S, Priyadharshini M, Gopinath K. SARS-CoV-2 - Understanding for the Preparation of Forthcoming Corona Virus Outbursts. Abasyn Journal of Life Sciences. 2020; 3(1):46-55. Google Scholar
- Wang W, Tang J, Wei F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J Med Virol. 2020 Apr;92(4):441-447.https://dx.doi.org/10.1002/jmv.25689 PubMed | Google Scholar
- Lone SA, Ahmad A. COVID-19 pandemic - an African perspective. Emerging Microbes & Infections. 2020 Jan 1;9(1):1300-8. https://doi.org/10.1080/22221751.2020.1775132. Google Scholar
- Giudicessi JR, Roden DM, Wilde AAM, Ackerman MJ. Genetic susceptibility for COVID-19-associated sudden cardiac death in African Americans. Heart Rhythm. 2020 Sep;17(9):1487-1492.https://dx.doi.org/10.1016/j.hrthm.2020.04.045 PubMed | Google Scholar
- Dyer O. Covid-19: Africa records over 10 000 cases as lockdowns take hold. BMJ. 2020 Apr 8;m1439.https://doi.org/10.1136/bmj.m1439 . Google Scholar
- Parker A, Koegelenberg CFN, Moolla MS, Louw EH, Mowlana A, Nortjé A, Ahmed R, Brittain N, Lalla U, Allwood BW, Prozesky H, Schrueder N, Taljaard JJ. High HIV prevalence in an early cohort of hospital admissions with COVID-19 in Cape Town, South Africa. South African Medical Journal. 2020 Aug 21;110(10):982-7.http://dx.doi.org/10.7196/samj.2020.v110i10.15067 . Google Scholar
- S Sigel K, Swartz T, Golden E, Paranjpe I, Somani S, Richter F, De Freitas JK, Miotto R, Zhao S, Polak P, Mutetwa T, Factor S, Mehandru S, Mullen M, Cossarini F, Bottinger E, Fayad Z, Merad M, Gnjatic S, Aberg J, Charney A, Nadkarni G, Glicksberg BS. Coronavirus 2019 and People Living With Human Immunodeficiency Virus: Outcomes for Hospitalized Patients in New York City. Clin Infect Dis. 2020 Dec 31;71(11):2933-2938.https://dx.doi.org/10.1093/cid/ciaa880 PubMed | Google Scholar
- Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa. Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin Infect Dis. 2021 Oct 5;73(7):e2005-e2015. https://doi.org/10.1093/cid/ciaa1198 PubMed | Google Scholar
- World Health Organization. Clinical features and prognostic factors of COVID-19 in people living with HIV hospitalized with suspected or confirmed SARS-CoV-2 infection, 15 July 2021. World Health Organization. 2021. Accessed Feb 2022. Google Scholar
- Chanda D, Minchella PA, Kampamba D, Itoh M, Hines JZ, Fwoloshi S, Boyd MA, Hamusonde K, Chirwa L, Nikoi K, Chirwa R, Siwingwa M, Sivile S, Zyambo KD, Mweemba A, Mbewe N, Mutengo KH, Malama K, Agolory S, Mulenga LB. COVID-19 Severity and COVID-19-Associated Deaths Among Hospitalized Patients with HIV Infection - Zambia, March-December 2020. MMWR Morb Mortal Wkly Rep. 2021 Jun 4;70(22):807-810. https://doi.org/10.15585/mmwr.mm7022a2 PubMed | Google Scholar
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, the Northwell COVID-19 Research Consortium, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, Hirschwerk DA, Kim EJ, Kozel ZM, Marrast LM, Mogavero JN, Osorio GA, Qiu M, Zanos TP. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. 2020 May 26;323(20):2052-9.https://doi.org/10.1001/jama.2020.6775 Google Scholar
- Collins LF, Moran CA, Oliver NT, Moanna A, Lahiri CD, Colasanti JA, Kelley CF, Nguyen ML, Marconi VC, Armstrong WS, Ofotokun I, Sheth AN. Clinical characteristics, comorbidities and outcomes among persons with HIV hospitalized with coronavirus disease 2019 in Atlanta, Georgia. AIDS. 2020 Oct 1;34(12):1789-1794. https://doi.org/10.1097/qad.0000000000002632 PubMed | Google Scholar