Outbreak Investigation and Enhanced Contact Tracing of Novel Coronavirus Disease 2019 (COVID-19), Ablekuma North Municipality, Greater Accra, Ghana
Anthony Baffour Appiah1, Benedict Calys-Tagoe2,&, Gyesi Razak Issahaku1, Delia Akosua Bandoh1, Charles Lwanga Noora1, Samuel Dapaa1, Charlotte-Alberta Cato3, Donne Kofi Ameme1, Ernest Kenu1
1Ghana Field Epidemiology and Laboratory Training Program (GFELTP), School of Public Health, University of Ghana, Legon- Accra, Ghana, 2Department of Community Health, University of Ghana Medical School College of Health Sciences, University of Ghana, Legon-Accra, Ghana, 3Ablekuma North Municipal Health Directorate, Ghana Health Service, Accra, Ghana, Accra, Ghana
&Corresponding author
Benedict Calys-Tagoe, Department of Community Health, University of Ghana Medical School College of Health Sciences, University of Ghana, Legon-Accra, Ghana. calys75@hotmail.com
Introduction:
After Ghana recorded its first two cases of COVID-19, other cases were subsequently identified in other parts of the country. The Ablekuma North Municipal Health Directorate was notified of a resident who reported to Korle-Bu Teaching Hospital on March 29, 2020 with fever, shortness of breath, general weakness, cough, chest pain. We investigated the report to estimate the magnitude of cases, to determine the secondary infection rate and to institute control and preventive measures.
Méthodes:
We conducted active case search using Ghana Health Service interim guideline for COVID-19 case investigation and management in Ablekuma North Municipality from April-July 31, 2020. We interviewed and collected samples of contacts and at-risk groups in affected households using collector for ArcGis and case investigation form. We summarized information of COVID-19 cases on our line list after samples have been confirmed. We analyzed data using Microsoft Excel 2016 and Stata 15, and presented as frequency and proportions.
Résultats:
The municipality recorded 213 cases with four deaths (Case fatality Rate=1.88%). The attack rate was 111.47 per 100,000 (213/ 191,075). Males were 135 (63.38%). The median age of case-patients was 27 years (interquartile range: 19 - 36years). Majority were students; 64 (30.05%). Most of the cases 89.20% (190/213) were asymptomatic. The median time between sample collection and release of laboratory results was 15 days (range: 4 - 22days). This response was a multi-sectorial approach, involving the Ministry of Health and the Ghana Health Service, Municipal Assembly, National Security Ministry, Ministry of Communication, Ministry of Information, and other government agencies.
Conclusion:
All confirmed cases were investigated. The attack rate was relatively high but low case fatality rate in the municipality. Strengthening laboratory capacity to test, to early report results is recommended. Lessons in handling cases indicate the need to sustain multi-sectorial collaboration to fight the outbreak.
Introduction

The Novel Coronavirus Disease 2019 (COVID-19) is a viral infection that spread mainly through air droplets [1]. The emergence and sporadic spread of COVID-19 from Wuhan City, China has threatened global health [2-4]. The commonest clinical features include fever, cough, acute respiratory distress, reduced or normal white blood cells, fatigue, and failure to resolve over 3 to 5 days of antibiotic treatment [5].
On March 12, 2020, Ghana recorded its first two cases of COVID-19. As of July 31, 2020, the Ghana Health Service had recorded 35,142 confirmed cases, 31,286 recoveries with 175 deaths [
6]. These cases spread across all the 16 administrative regions in the country with disproportionate distribution (above 80%) in Greater Accra, national capital [
6]. Prudent measures have been implemented to prevent and control the importation of cases from foreign countries, rigorous contact tracing, and testing of samples from contacts. However, the local transmission remains a challenge.
In line with the national preparedness strategy for the global pandemic [
7], the Ablekuma North Municipal Health Directorate (MHD) instituted a number of measures and plans to adequately contain the outbreak. These included organizing series of stakeholder consultative meetings, building the capacity of local health staff through COVID-19 sensitization and refresher training, strengthening routine surveillance in health facilities among others. The MHD allocated rooms to be used to temporarily quarantine suspected cases, and drugs to initially manage any presentation until laboratory confirmation and subsequent isolation at the National Case Management Center.
On March 29, 2020, a 71 years old man who resides in Kwashieman, a suburb of Ablekuma North Municipality, reported to Korle-Bu Teaching Hospital (KBTH) with history of fever, shortness of breath, general weakness, cough, chest pain and a travel history (he had returned from the United Kingdom 14 days prior to presentation). The facility suspected, collected and tested nasopharyngeal sample for COVID-19 as part of their routine surveillance, his result came out positive for COVID-19. On receiving the results, KBTH notified the Ablekuma North Municipal Health Directorate, Greater Accra region, Ghana, which constituted an outbreak investigation team to immediately respond to the event. We investigated the outbreak to estimate the magnitude of cases, to determine the secondary infection rate and to institute control and preventive measures.
Methods

Outbreak Setting
The Ablekuma North Municipality is in the Greater Accra Region, Ghana. The municipality has five sub-municipalities namely Kwashieman, Odorkor, Awoshie, South Odorkor, and
Darkuman. The Municipality has a projected population of 191,076 in 2020 based on the 2010 population and housing census with 92,672 males and 98,404 females [
7]. The municipality has no public hospital but has 15 functional Urban Community-based Health Planning and Services (CHPS) zones which provides home visit and CWC services to their catchment area. The municipality is cosmopolitan in nature and serves as home for people from diverse ethnic backgrounds. Economic activities in the municipality are mainly commercial/services, trading and local industrial activities with some major markets like Mallam and Odorkor markets which facilitate high level of person-to-person interaction in the municipality. At the time of this investigation, March 29, 2020, the municipality was among forty-five districts fighting the COVID-19 outbreak with two COVID-19 cases confirmed.
Data collection
Prior to field investigation and data collection, a series of trainings were organized for health personnel identified to participate in the contact tracing activities after debriefing at directorate. The training focused on key protocols in contact tracing, and sample collection mainly on the use of collector for ArcGIS, and Surveillance Outbreak Response and Management Analysis System (SORMAS) [
8].
A line list of COVID-19 case-patients was obtained to establish the community and exact residential locations of cases. The affected case-patients were initially visited at their home for ono-on-one interview and sample collection of primary contacts before isolation was done. Follow up phone interviews were also conducted for some contacts. Data was captured with paper-based case-investigation forms, SORMAS and ArcGIS. These were synchronized with the nationwide database. At the municipality, we summarized details of samples taken on a line list for easy tracking those who tested positive. These included age, sex, signs and symptoms, chronic medical condition, date sample was taken, community sample was taken from, date results was received, date of discharge, treatments given and outcome. We recorded the place of residence of all the case-patients and their contacts using SORMAS and ArcGIS software downloaded onto a portable mobile device.
Enhanced contact tracing
In order to contain the outbreak during the early stages, we embarked on enhanced contact tracing in all communities and public places in the municipality between 1st and 25th April, 2020. Enhanced contact tracing is a rigorous public health approach in identifying contacts of case-patients and persons at risk, collecting and testing samples, isolating and treating infected persons to effectively reduce the spread of infection in the population [
1]. This took place in two phases. In phase I, teams of contact tracers were distributed within a 2-kilometer radius of houses with confirmed cases.
The collector for ArcGIS was used to pick GPS coordinates of each household visited. In the phase II, teams were sent to commercial areas and public places to identify and sample traders, food venders, commercial sex workers, and commercial drivers. We collected sputum samples or nasopharyngeal swabs from each contacts of cases and at risk groups interviewed between 1st and 25th April, 2020. They were also advised to stay at home till results released to them. Variables collected during interview included age, sex, occupation, exposure history, sign and symptoms, chronic medical condition, date sample was taken, and household details such as household head name and contact, household size, and number sleeping rooms.
Laboratory investigation
Samples taken included sputum and nasopharyngeal swabs for laboratory investigations. On the field, samples were collected in plastic containers and packed into sample carriers to the sample collation center at the health facility. After sample collation from contact tracing teams, we employed triple packaging technique to package and transport the samples to the Noguchi Memorial Institute for Medical Research (NMIMR) of the
University of Ghana, and the National Public Health Reference Laboratory (NPHRL) at Korle-Bu Teaching Hospital for processing and analysis.
Data analysis
Data captured during active case search and enhanced contact tracing were entered and analyzed descriptively using Excel (Microsoft Excel 2016) and Stata (Stata IC 15). We performed univariate analysis and expressed categorical variables as frequencies and percentages. Continuous variable (age) was expressed as median and interquartile range (IQR). We summarized the data in terms of time, place and person. The overall attack rate was calculated among the general population based on the projected population by Ghana Statistical Service (GSS) for Ghana Health Service (GHS) [
7]. We also drew an epidemic curve to show the distribution of the case-patients in the community by date sample was taken.
Ethics declarations
Permission to use data for this report was obtained from the National Disease Surveillance Unit and the health directorate of Ablekuma North Municipality. During our community sample collection, consent of cases and contacts were verbally obtained and were assured of data confidentiality and anonymity.
Results
Descriptive Epidemiology
As of July 31, 2020, a total of 3241 contacts were traced with their samples taken. The median time from sample collection to release of laboratory results was 15 days (range: 4 - 22days). Of 3241 contacts, 213 were confirmed positive with COVID-19 while four deaths were recorded. The overall attack rate between March 29, and July 31, 2020 was 111.47per 100,000 population (213/191,075) with a Case Fatality Rate of 1.88% (4/213). Majority of the cases were males (63.38%, 135/213) with a male to female ratio of 1.7:1. The median age of case-patients was 27 years (IQR: 19 -36years). The most affected age group was 20-29 years (25.82%, 55/213), followed by 10-19 years (24.41%, 52/213). Majority of the case-patients were students (30.05%, 64/213) whereas only 7.98% were health workers. Cases were reported from all the five sub-municipalities with the majority (28.64%, 61/213) in South Odorkor sub-municipality
Table 1.
Most (89.20%, 190/213) of the cases were asymptomatic with only 5.16% (11/213) presenting with COVID-19 symptoms. The commonest symptoms experienced by the case- patients were cough (63.64%, 7/11), fever/chills (45.45%, 5/11), and shortness of breath (36.36%, 4/11) while three (27.27%, 3/11) case-patients had runny nose. Three cases had chronic underlying medical conditions (one diabetic and two hypertensives)
Table 2.
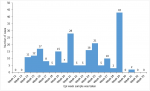
On March 29, 2020, the municipality reported its first case followed by 10 cases till April 4, 2020 (in epi week 14), the cases peaked on in week 29 (July 12-18, 2020) with 43 cases. The epidemic curve indicates an intermittent exposure mainly through secondary transmission (person-to-person)
Figure 1.
Case management
All confirmed case-patients detected via routine surveillance were sent to the National Case Management Centre (NCMC) and managed according to severity of symptoms. Case-patients confirmed through contact tracing were initially managed on oral Azithromycin (500mg), Vitamin C (500mg), and Zinc Tablet (50mg) before they were isolated to NCMC. As at July 31, 2020, there were two active cases (0.94%), 157 (73.71%) had been discharged for home management, 50 (23.47%) had recovered with four (1.88%) deaths
Table 2. The summary of fatalities is shown in
Table 3. Only one case died who had history of fever, cough, shortness of breath and underlying medical conditions (diabetes and hypertension).
Coordination and multi-sectoral collaboration
The response to the outbreak was through multi-sectoral collaboration.
Table 4 indicates response component, key activities and sectors or agencies involved. The sectors involved in this response included the Ministry of Health, Ministry of Education, National Security Ministry, Ministry of Communication, Ministry of Information, Ministry of Local Government and Rural Development. The Municipal Assembly and the Security agencies ensure residents complied with the ban on public and social gatherings, enforcement of face mask use and social distancing protocol and pick-up schedules for cases in the communities. Three ministries; health, communication and information provided platform to education and update the population on the COVID-19 situation, enhanced contact tracing, COVID-19 protocols and others strategies in place to address the pandemic. At the municipal level, Municipal Health Management Team (MHMT) constituted a team made up of the MHMT, the hospital staff, the Municipal Assembly, Ghana Ambulance Service, Ghana Immigration service, Ghana Police Service and the Ghana Education Service. On the field, the investigation team called on the Municipal Assembly to facilitate police enforcement to ensure cooperation between members of affected communities and the contact tracing teams when necessary. As part of the case management protocol, the Ghana Health Service (i.e. the MHMT) collaborated with the Ghana Ambulance Service and the National Security Ministry to pick cases from their respective communities to NCMC.
Laboratory investigations
A total of 3241 samples (sputum 2306(99.10%) and nasopharyngeal swabs 21(0.90%)) were taken, packaged and transported to NMIMR. The laboratory communicated 213 confirmed COVID-19 cases as at July 31, 2020, representing a positivity rate of 6.57%.
Enhanced contact tracing
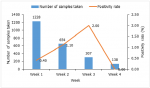
A total of 2202 contacts were traced from communities and public places in the municipality between 1st and 25th April, 2020 (88.56% (1950/2202) were through community screening, and 10.99% (242/2202) were primary contacts of confirmed cases). Most of the contacts 52.77% (1228/2202) were traced in week 1 of the enhanced contact tracing activities with the least number of contacts 6.27% (138/2202) in week 4. The overall positivity rate during the period of enhanced contact tracing was 0.82% (18/2202) and positive rate peaked (2.00%) in week 3 (6/307)
Figure 2.
Discussion
The emergence and sporadic spread of COVID-19 remains a threat to global health, economic and socio-cultural wellbeing. Although, prudent measures were implemented to prevent importation of cases of COVID-19 in Ghana, we could not entirely stop importation which translated to community transmissions. This informed our COVID-19 outbreak investigation and enhanced contact tracing at the Ablekuma North Municipality in line with Ghana´s Ministry of Health Provisional Standard Treatment Guidelines for COVID-19 [8].
Our investigation and enhanced contact tracing detected 213 COVID-19 cases and 4 deaths between March 29, 2020 and July 31, 2020. The overall attack and case fatality rates were estimated to be 111.47 per 100,000 population and 1.88% respectively. The attack rate in the municipality was comparable to estimated national figure (113.36 per 100,000; 35142/31,000,000) but the CFR was much higher than the national average (0.49%, 175/ 35142) [
6]. This could be explained by undue delay in releasing test results and isolating confirmed cases to the National Case Management Center as the median time of releasing results was 15 days (range: 4 - 22days). It was also observed that people suspected to have been infected with the virus present to the health facility at later stages, thereby influencing the outcome of management.
Although previous reports suggested that clinical presentations of COVID-19 are commonly reported in older populations [
9,
10], we found a younger median age of 27 years with a range between 6 years and 89 years. The median age of our case-patients was almost half of the 47.5 years (between 1 year and 94 years) reported from China [
9]. By age stratification, the most affected population were below 40 years (73.2%) which comprised of cases within 10-39 years. This age pattern was also younger than what had been reported from previous studies [
8,
9]. The younger case-patients recorded in this study could be explained with the demography of Ghana, which has a youthful population [
10]. The high mobility and direct physical interactions among the youth might further explained the high incidence among younger age groups. Also, during our field investigation we observed that the youth mainly, were not adhering to the use of face mask and to social distancing protocol which might have promoted person-to-person spread in younger population.
In this study, males were more affected (63.38%) with male to female ratio of 1.7:1. Similar a higher proportion of males was reported in systematic study [
8]. In contrast, another study observed more of the COVID-19 cases to be females (51.2%) [
9]. On occupation of case-patients, majority of them were students (30.05%) followed by traders (14.08%). The higher representation of students depicts how ruthless the spread of the COVID-19 among the youthful populations in the municipality and Ghana. The spread of the COVID19 among students was facilitated by their resumption to school to complete their academic activities. Further analysis on the students´ demographic data indicated that 59.37% (38/64) of our student cases were detected in the school from July 6th to 15th, 2020. This was the period the final year Senior High School students were called back to complete their preparations for the West African Senior Secondary Certificate Examination (WASSCE).
Although there was an increased infection rate among frontline health workers, only seventeen (7.98%) of our cases were frontline health workers. The frontline health workers in the Municipality adhered strictly to COVID-19 safety protocols while using standard personal protective equipment, most often, at their own cost. This might have accounted for the low infection rate among the frontline health workers. Previous study in Ghana indicated that due to internal migration between the hotspots and other regions COVID-19 cases have been reported in all the 16 administrative regions [
11]. Similar observations were made in the present study where cases were reported from all the five sub-municipalities in the Ablekuma North Municipality. We observed that cases were frequently reported from South Odorkor, Kwashieman, and Odorkor sub-municipalities. We addressed the incidence in these municipality by intensifying our enhanced contact tracing with more teams, ensured early isolation, health education and risk communication.
A significant proportion of the cases were asymptomatic while only eleven of the case-patients presented with cough, fever, chills, and shortness of breath. Consistent with our report on symptoms, fever and cough were the most common presentation among case-patients in Ghana [
11] and China [
8,
9]. High level of asymptomatic cases in our setting corroborates with previous studies from Ghana [
11], United States [
12] and Germany [
13]. Compared with our findings, a systematic review reported much lower pooled prevalence of COVID-19 asymptomatic infection of 15.50% [
8]. Although the exact explanation to the high proportion of asymptomatic cases is yet be documented in Ghana, we opined that, early detection and management, a younger and active populations, as well as adoption of healthy eating and regular exercise are potential protective factors limiting the progression of the infection. The strategy of enhanced contact tracing ensured that individuals were diagnosed at an early stage of the disease and managed. This could also have contributed to the high proportion of asymptomatic individuals.
The epidemic curve in this study showed an intermittent exposure mainly through a secondary transmission (person-to-person). The cases in the municipality peaked on epi week 29 with 43 cases. The incubation period of COVID-19 (i.e. the time between exposure to the virus and symptoms onset) according to the World Health Organization is between 2 and 14 days [
1]. It was difficult to estimate the incubation period among our study participants, since a greater proportion of our cases who were asymptomatic could not recall their exposure history. The “date of sample taken” in the case of this study was problematic and inconsistent to represent the actual date of onset of illness/symptoms. For instance, a systematic review reported that nearly half of the patients who were diagnosed with COVID-19 asymptomatically at screening time might be in their incubation period and develop symptoms later [
8], although, none of our asymptomatic cases later developed symptoms of COVID-19.
The positivity rate in the municipality was 6.57%. With an average time from sample collection to release of laboratory results at 7days usually between 4 days and 22days. The delay in testing and release of results is a challenge and could promote further transmission. Response to COVID-19 outbreak should be rapid to stop person-to-person transmission, and most importantly when nearly 90% of our cases were asymptomatic with most samples collected through community surveillance. Increased testing capacity in the country could be the core in addressing unnecessary delays in result communication.
All confirmed case-patients were sent to National Case Management Centre (NCMC) and managed according to the Ghana Ministry of Health and the WHO COVID-19 case management guidelines [
7,
14]. Although response to outbreak was through multi-sectoral collaboration, we faced some difficulties managing confirmed cases from the communities. This was partly due to delays by the National Case Management Team (NCMT) to isolate cases from their houses especially when self-isolation was impossible. In some instances, cases failed to comply with pick-up guidelines. As at July 31, 2020, the municipality had two active cases, 157 discharged but under home management, 50 had fully recovered with four deaths. Contrary to the Ghana national epidemiological data of COVID-19 related deaths, our data suggest that, only one of our fatalities had history of diabetes mellitus and hypertension [
6]. The difference in proportion of chronic medical conditions reported at the national and district level could be attributed to population dynamics, knowledge of having the condition, and differences in accuracy in documenting case-patients information from reporting sites.
Limitations
Our study was limited by missing data identified for some cases captured on the municipality line list. This was because some confirmed cases were not cooperating with investigation team. This might have affected the true representation of selected variables in this study. Most of our cases could not recall their exposure history making it difficult to estimate the actual mean duration of exposure. Nonetheless, our study revealed vital information that informed risk communication and prevention strategies in the municipality and the Country at large. The study also provided preliminary data to inform further epidemiological studies among cases in the municipality.
Conclusion
The Ablekuma North Municipal had recorded 213 COVID-19 cases with four fatalities between March 29 and July 31, 2020. This represented an attack rate and case fatality rate of 111.47 per 100,000 and 1.88% respectively. The delay in testing and results communication affected case isolation and pick-up from affected communities. This outlined the need to strengthen laboratory capacity to test and early report results. Lessons in handling cases indicate the need to sustain multi-sectorial collaboration to fight the outbreak. We also recommend the Ministry of Health and Ghana Health Service (GHS) with partners to intensify public education and sensitization of COVID-19 safety protocols. Also, the GHS should address data quality issues which include missing data.
What is known about this topic
- The emergence and sporadic spread of COVID-19 remains a threat to global health, economic and socio-cultural wellbeing
- The commonest clinical features include fever, cough, acute respiratory distress, headache, fatigue, and many others
- COVID-19 has affected all the 16 administrative regions in Ghana with disproportionate distribution (above 60%) in Greater Accra, national capital
What this study adds
- This study estimated the magnitude of cases and the secondary infection rate of COVID-19 in one of the hotspot municipalities in the Greater Accra Metropolis of
Ghana
- COVID-19 outbreak response is through multi-sectoral collaborative approach
- The high asymptomatic COVID-19 in younger population is due to non-adherence to face mask and social distancing COVID-19 protocols among youths
Competing interests
The authors declare no competing interests.
Authors' contributions
ABA, CAC, EK, BCT, CN, RG, DB, SD and DA supported the outbreak investigation and enhanced contact tracing. ABA conceived the idea, framed the design, performed statistical analysis, drafted and revised the initial manuscript. CAC, BCT, EK, CT, CN, RG, DB, SD, and DA were involved in write-up, edited and reviewed the manuscript. The author(s) read and approved the final version of this manuscript.
Acknowledgements
Authors acknowledge the support of National Surveillance Department of the Ghana
Health Service, USA Center for Diseases Control and Prevention (CDC), African Field
Epidemiology Network (AFENET), and Ghana Field Epidemiology and Laboratory Training Programme (GFELTP) for their technical and financial support. We wish to express our gratitude to the Municipal Health Management Team (MHMT) Ablekuma North Municipality Health Directorates for their support and warm reception, and our hardworking contact tracers who worked tirelessly to identified and traced contacts in the municipality.
Tables and figures
Table 1: Socio-Demographic Characteristics of confirmed COVID-19 cases, Ablekuma North Municipal, March-July, 2020
Table 2: Clinical characteristics of Confirmed COVID-19 cases, Ablekuma North Municipal, March-July, 2020
Table 3: Epidemiological characteristics of COVID-19 deaths recorded, Ablekuma North Municipal, March-July, 2020
Table 4: Multi-sectoral collaboration in COVID-19 response, Ablekuma North Municipal, March-July, 2020
Figure 1: Epidemic curve of the COVID-19 outbreak in Ablekuma North Municipality, March-July, 2020
Figure 2: Cumulative samples taken and Positivity rate, Ablekuma North Municipality, 1st - 25th April 2020
References
- WHO. Coronavirus disease 2019. WHO. 2020. Accessed Dec 2021.
- Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, Li J, Zhao D, Xu D, Gong Q, Liao J, Yang H, Hou W, Zhang Y. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020; 395(10226):809-815. https://doi.org/10.1016/S0140-6736(20)30360-3 PubMed | Google Scholar
- Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, Ren R, Leung KSM, Lau EHY, Wong JY, Xing X, Xiang N, Wu Y, Li C, Chen Q, Li D, Liu T, Zhao J, Liu M, Tu W, Chen C, Jin L, Yang R, Wang Q, Zhou S, Wang R, Liu H, Luo Y, Liu Y, Shao G, Li H, Tao Z, Yang Y, Deng Z, Liu B, Ma Z, Zhang Y, Shi G, Lam TTY, Wu JT, Gao GF, Cowling BJ, Yang B, Leung GM, Feng Z. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. 2020 Mar 26; 382(13):1199-1207. https://doi.org/10.1056/nejmoa2001316 PubMed | Google Scholar
- Zhao D, Yao F, Wang L, Zheng L, Gao Y, Ye J, Guo F, Zhao H, Gao R. A comparative study on the clinical features of COVID-19 pneumonia to other pneumonias. Clin Infect Dis. 2020 Jul 28; 71(15):756-761.https://doi.org/10.1093/cid/ciaa247 Google Scholar
- Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med (Lond). 2020 Mar; 20(2):124-127. https://doi.org/10.7861/clinmed.2019-coron PubMed | Google Scholar
- GHS. COVID-19 Updates Ghana. GHS. 2020. Accessed Dec 2021.
- Ghana Statistical Service (GSS). 2010 Population and Housing Census: Regional Report Central Region. GSS. 2013. Accessed Dec 2021.
- Ghana Ministry of Health. . Republic of Ghana Ministry of Health Provisional Standard Treatment Guidelines for Novel Coronavirus Infection COVID - 19 Guidelines for Ghana. Ghana, MOH. 2020. Accessed Dec 2021.
- He J, Guo Y. Proportion of asymptomatic coronavirus disease 2019: A systematic review and meta-analysis. J Med Virol. 2020; 15:1-24.https://doi.org/10.1002/jmv.26326 . Google Scholar
- Tian S, Hu N, Lou J, Chen K, Kang X, Xiang Z, Chen H, Wang D, Liu N, Liu D, Chen G, Zhang Y, Li D, Li J, Lian H, Niu S, Zhang L, Zhang J. Characteristics of COVID-19 infection in Beijing. J Infect. 2020; 80(4):401-406.https://doi.org/10.1016/j.jinf.2020.02.018 PubMed | Google Scholar
- A Odikro M, Kenu E, L Malm K, Asiedu-Bekoe F, L Noora C, L Noora C, Frimpong J, Calys-Tagoe B, A Koram K. Epidemiology of COVID-19 outbreak in Ghana, 2020. Ghana Med J. 2020; 54(4):5-15.https://doi.org/10.4314/gmj.v54i4s.3 . Google Scholar
- Roxby AC, Greninger AL, Hatfield KM, Lynch JB, Dellit TH, James A, Taylor J, Page LC, Kimball A, Arons M, Munanga A, Stone N, Jernigan JA, Reddy SC, Lewis J, Cohen SA, Jerome KR, Duchin JS, Neme S. Outbreak Investigation of COVID-19 Among Residents and Staff of an Independent and Assisted Living Community for Older Adults in Seattle, Washington. JAMA Intern Med. 2020; 180(8):1101-1105.https://doi.org/10.1001/jamainternmed.2020.2233 . PubMed | Google Scholar
- Böhmer MM, Buchholz U, Corman VM, Hoch M, Katz K, Marosevic DV, Böhm S, Woudenberg T, Ackermann N, Konrad R, Eberle U, Treis B, Dangel A, Bengs K, Fingerle V, Berger A, Hörmansdorfer S, Ippisch S, Wicklein B, Grahl A, Pörtner K, Muller N, Zeitlmann N, Boender TS, Cai W, Reich A, an der Heiden M, Rexroth U, Hamouda O, Schneider J, Veith T, Mühlemann B, Wölfel R, Antwerpen M, Walter M, Protzer U, Liebl B, Haas W, Sing A, Drosten C, Zapf A. Investigation of a COVID-19 outbreak in Germany resulting from a single travel-associated primary case: a case series. The Lancet Infectious Diseases. 2020; 20(8):920-928.https://doi.org/10.1016/S1473-3099(20)30314-5 Google Scholar
- WHO. Clinical management of COVID-19: interim guidance, 27 May 2020. WHO. 2020. Accessed Dec 2021. Google Scholar