Maternal choices of delivery sites among recently delivered women in Liberia, 2017
Gabriel Boumen Kassay1, Ben Gbouh1, Dedesco Gweh1, Emmanuel Dweh1, Emmanuel Ghartey1, Felecia Dweh1, Lawrence Larway1, Leroy Maximore1, Moses Fomba1, Sylvester Toe1, Tamba Alpha1, Faith Whesseh1, Roseline George1, Trokon Yeabah1, Olayinka Stephen Ilesanmi2, Peter Adewuyi2, Fulton Shannon II2, Wede Himiede Wilson2,&, Obafemi Babalola2, Thomas Nagbe2, Maame Amo-Addae2
1Liberia Field Epidemiology Training Program, Monrovia, Liberia, 2Africa Field Epidemiology Network, Liberia
&Corresponding author
Wede Himiede Wilson, Liberia Field Epidemiology Training Program, Monrovia, Liberia. whwhimwil3@yahoo.com
Introduction:
To reduce maternal mortality, many countries encourage women to deliver in health facilities, where complications can be handled more effectively. In Liberia, attempted home deliveries accounted for about 10% of maternal deaths in 2016/2017. It is therefore necessary to identify the factors influencing maternal choice of delivery site in Liberia. This study seeks to determine the preferred choice of delivery site and factors associated with the choice in Liberia.
Methods:
A cross-sectional design was used to study 630 women of reproductive age who had given birth less than one year before the survey. A two-stage cluster sampling
method using a modified WHO 30 by 7 approach was used to select 30 communities (clusters) and 21 women within each cluster as respondents. A pre-tested interviewer-administered semi-structured questionnaire was used.
Results:
The mean age of study participants was 26 ± 6.8 years, with 84% between 18 and 35 years. The median number of births per woman was 5 (1 - 12). The proportion of mothers who preferred health facility over home delivery as their original choice of delivery site was 86%, four times greater than those who preferred home over health-facility delivery (22%), (POR= 3.8, 95% CI: 1.6 – 9.1). Mothers who attended < 4 antenatal visits were 30% less likely to originally choose health facilities as their preferred delivery site compared to those who had 4 or more antenatal visits (60% vs 86%) (POR= 0.7, 95% CI: 0.5 – 0.9). Women living in communities where the leaders had instituted sanctions against women who deliver at home were 10% more likely to choose health facility delivery, compared to those whose communities had no sanctions (POR= 1.1, 95% CI: 1.0 – 1.2).
Conclusion:
Health-facility deliveries are preferred to home deliveries. County Health Teams should sensitize the community on the benefits of delivering at the health facility and increase community involvement (local authorities).
Introduction

Globally, an estimated 830 women die everyday from pregnancy- or childbirth-related complications [1]. Most of the deaths occur in low-resource settings in developing countries. In 2015, the maternal mortality ratio in developing countries was 239 per 100,000 live births, higher than the sustainable development goal target of 70/100,000 live births and the 12/100,000 in developed countries [1]. More than half of the deaths in developing countries occurred in Sub-Saharan Africa and could have been prevented [2]. Skilled care before and during delivery improve the outcome of pregnancy [3, 4].
The maternal mortality ratio (MMR) in Liberia was 1072/100,000 live births in 2013 [
5]. The 2013 Liberia Demographic Health Survey (LDHS) showed that a little under half of births (44%) occurred outside health facilities, with only six in ten births assisted by a skilled provider. Home deliveries were more common in rural areas (54%) than urban areas (34%), and women with more education and those from wealthier families were more likely to have their births attended to by a skilled provider [
3]. In Liberia, home deliveries are commonly conducted by traditional midwives, who are unskilled attendants. A rapid retrospective analysis of maternal deaths which had occurred within the six months prior to this study revealed that at least 10% of these cases either had home delivery or had attempted home delivery.
In keeping with the Ministry of Health directive in 2015 to classify maternal death as a priority event requiring surveillance, the National Public Health Institute of Liberia (NPHIL) has focused on maternal deaths to institute appropriate interventions. Residents of the Liberia Intermediate Field Epidemiology Training Program (LFETP-I) Cohort 1 designed and conducted a survey to provide a better understanding of why women chose home delivery over facility delivery in Liberia. The study also sought to assess factors associated with choice of delivery site. The results are intended to be used by the Liberia Ministry of Health (MOH) to develop appropriate interventions to reduce home deliveries for improved pregnancy outcomes and maternal health.
Methods

Study setting
Liberia is in the Western coast of Africa, bounded on the West by Sierra Leone, East by Côte d´Ivoire, North by Guinea and on the South by Atlantic Ocean. It covers an area of 111,370 Square kilometres. Liberia has an estimated population of 4.7 million inhabitants with a growth rate of 2.1% projected from the National Housing and Population Census of 2008. Of the total population: 4.3% are under one, 17% are under 5 and 45% under 15 years. Population density is around 37 per square km, but very uneven, with four counties hosting 70% of the total population. The rural regions are home to an estimated 53% of the population. Administratively, Liberia is sub-divided into 5 Regions, 15 Counties and 91 health districts. Christians made up 95% of Liberian´s population [
6]
Study Design
We conducted a national cross-sectional cluster survey. The study population were women who had delivered within one year prior to the survey.
Sample size estimation
The sample size for the survey was calculated using Epi Info 7 [
4]. The estimated size of the target population was 800,000 women in reproductive age since women of childbearing age constitute approximately 23 percent of Liberia´s 3.5 million population [
7]. The expected health-facility delivery frequency was 56% [
5]. We used a confidence interval of 95%, and design effect of 1.5 to account for cluster sampling and obtained a sample size of 568. We applied a non-response margin of 10% to obtain an adjusted sample size of 624.
For the purpose of this survey, we modified the WHO 30 by 7 cluster into a 30 by 21 cluster survey. This gave us a total sample size of 630.
Sampling Technique
A two-stage cluster sampling was done to obtain our sample of respondents.
Stage 1: We selected 30 communities in Liberia using simple random sampling method. Each community selected was defined as our clusters.
Stage 2: Within each cluster, 21 respondents were selected. To select the respondents, we conducted house-to-house visits, starting from the house closest to the home of the head of the community. In each house, we enquired from the residents if any woman had delivered a baby within a year. All women in the house who had delivered a baby within a year were included in the study if they gave consent. (The nearest house to the starting house was visited next?). From each selected house, the next house was the nearest house, a process which was repeated until the required number of respondents (21 per community cluster) was achieved. Delivery status of the women were obtained from the history provided by the residents of the home and by the women.
Inclusion and exclusion criteria
The study population for the survey were women who had delivered a baby in Liberia within the year preceding the study. Visitors and non-permanent residents of the community, and non-consenting eligible women were excluded.
Questionnaire and Variables
The questionnaire for the study was adapted from the Demographic Health Survey questionnaire. Questions were grouped into 5 categories: socio-demographic data, reproductive history, knowledge, utilization of maternal health care services and practices. The outcome variable was the initial choice of delivery site and final place of delivery.
The questionnaire was pre-tested to assess ambiguity and clarity of questions and was revised based on feedback from pretest.
We defined home delivery as the delivery of a baby in the home or in any other setting outside of a healthy facility. Health-facility delivery was defined as the delivery of a baby within a health facility, hospital, or clinic.
Data Collection
Respondents were interviewed and data was collected by the 14 residents of LFETP Cohort 1, comprising county and national surveillance officers. Field supervision was done by mentors of the Liberia Field Epidemiology Training Program.
Statistical Analysis
Data were cleaned, coded, and entered into the computer and analyzed using the Epi Info and SPSS statistical software [
8,
9].
Categorical variables (e.g., sex of respondents, occupation, educational level, household socioeconomic status, health care services utilized) were summarized as proportions and compared. Continuous variables (age of respondents, average monthly household income) were summarized as means with standard deviation or median with range.
The socio-economic status (wealth quintiles) index was developed using Principal Components Analysis (PCA) in SPSS. The input to the PCA was information on ownership of house and other key assets such as a stove, electric fan, refrigerator, air conditioner, radio, television, and generator, piped water in the household, bicycle, motor vehicle, upholstered chairs, sewing machine and washing machine. We used quintiles to calculate of distribution cut points. Each woman was assigned the wealth index score of her household, where Q1= Lowest, Q2=Second, Q3= Middle, Q4= Fourth, Q5=Highest.
Our findings are presented in prose, frequency tables and charts. Inferential statistics using prevalence ratios and chi-square test was done to test for associations between selected characteristics and outcome. Results were reported using unadjusted prevalence odds ratios (POR), confidence interval at 95% and level of statistical significance was set at 5%.
Ethical Considerations
Ethical approval to carry out the study was obtained from IRB, Liberia. The women were informed of their right to decline or withdraw from the study at any time without any adverse consequences. Written informed consent was obtained from the respondents, and those who could not provide a written signature were asked to thumbprint the consent form. Data collected was used only for survey purposes and kept confidential on a password-protected computer. Names and addresses were not included in the data collection instrument and thus collected data could not be linked to any person. Researchers were also trained to keep information confidential. The findings were communicated to the National Public Health Institute and the Ministry of Health, Liberia and advocacy efforts were instituted from the national to the county level.
Results
Key characteristics of respondents
The mean age of the 630 women interviewed was 26 years ± 6.8 years, and median age was 25 years (range; 14 years to 50 years). Thirty-five (6%) were below 18 years. Among the 443 who provided responses on income, the median monthly income was $30 (Range $1 - $2000). The median number of children the respondents had was 5 (range: 1 to 12). A total of 118 (19%) had experienced the death of a child. The other socio-demographic characteristics are shown in
Table 1.
Original and final choice of delivery site with reasons for change of delivery site
When asked about their original preferred choice of delivery site and where they finally/eventually had their delivery, 527 (84%) respondents originally chose to deliver at the health facility, and 103 (16%) at home. However, 517 (82%) eventually delivered at the health facility versus 113 (18%) at home. Of the 527 respondents who originally chose to deliver at the health facility, 499 (95%) maintained their choice and 28 (5%) eventually delivered at home. Also, 18 (17.5%) of those who originally chose to deliver at home eventually delivered at the health facility. Those aged 25 - 29 years (19.7%), traders (21.8%), farmers (15.9%), and those with elementary education (18.9%) had the highest proportions of respondents with the home as an original choice of delivery site
Table 2.
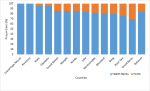
Overall, 527 (84%) of the respondents originally chose to deliver at the health facility
Figure 1. All respondents at Grand Cape Mount and Rivercess Counties chose the health facility as an original delivery site. However, Grand Bassa 13/42 (31%), River Gee 5/21 (24%), Bong 13/63 (21%) and Maryland 4/21 (19%) Counties were the four leading counties with relatively high proportions of respondents who chose the household as their original place of delivery. This is more than the national proportion of 103/630 (16%)
Figure 1.
The most common reasons for maintaining the original choice of health facility for delivery were: to receive good maternal, neonatal care and treatment 366 (73%), closeness of the health facility to respondents, and labour starting late at night 40 (8%). In addition, a total of 30 (6%) maintained their original choice of health facility because it was where they received antenatal care
Table 3. The 28 (5%) respondents who changed from original choice of health facility to finally deliver at home, believed that they would receive better care and treatment from the trained traditional midwives 6 (21%); had labour that was fast and started late at night 5 (18%); and had bad roads to or lived far from the hospital 4 (14%).
Among the 18 (17.5%) respondents who abandoned their original choice of home delivery for health facilities, 6 (33%) were referred to the health facility or had an emergency in the course of the pregnancy and delivered by caesarean section. Another 8 (44%) did so because they wanted good neonatal and maternal care. Overall, 85 (14%) of the respondents with home as the original choice of delivery site finally delivered there. The major reason for maintaining the original choice and finally delivering at home was the belief that respondents would receive better care from the trained traditional midwives in the community- 29 (34%). In addition, the long distance to the hospital, coupled with poor road conditions accounted for 19 (22%) respondents delivering at home. The fear of surgery and dislike for health facility staff, and cost of delivery were among the other reasons for home deliveries.
Benefits of antenatal visits and choice of delivery site
A total of 578 (93%) respondents said that there were benefits of attending antenatal check-ups at the health facility. Majority (92%) correctly identified that the first antenatal visit should be within the first three months of pregnancy. Also, 555 (92%) had had 4 or more antenatal visits while pregnant.
Of the 554 (88%) who knew of any benefits of health-facility delivery, 471 (85%) originally chose the health facility as a delivery site. From the 588 respondents who saw no benefits of delivering at home, 506 (86%) chose health facility as the original choice while 82 (14%) preferred the home as the original choice for delivery in spite of seeing no benefits in home delivery. Thirty - eight (6%) respondents said there were benefits of home delivery over health-facility delivery, five of which (13.2%) were displeased with unpleasant language used by health workers in addressing patients, and especially those who did not have enough money to pay for services; and the inability of health workers to keep their secrets.
When asked which was ‘better’, 612 (97%) women indicated health-facility delivery was better. However, among these, only 523 (85%) had the health facility as an original delivery site. A total of 18 (3%) respondents said home delivery was better than hospital delivery.
Among the 343 respondents aware of community sanctions against home delivery, 296 (86%) made the health facility their original choice of delivery site.
Factors associated with maternal choice of delivery site
The maternal factors associated with original choice of delivery site included the mothers´ judgement of which delivery site was better. The proportion of mothers who said health facility was better than home delivery and eventually delivered at health facility (86%) was 4 times greater than those who said home delivery was better (22%), {Prevalence Odds Ratio (POR)= 3.8,95% CI: 1.6 - 9.1}. Also, mothers who saw no benefits in home delivery (86%) were 2 times more likely to have the health facility as their original delivery site as compared to those who identified benefits of home delivery (45%), (POR= 1.9, 95% CI: 1.3 - 2.7). Mothers who attended < 4 antenatal visits were 30% less likely to choose the health facility as an original delivery site (60% vs 86%) compared to those who had 4 or more antenatal visits (POR= 0.7, 95% CI: 0.5 - 0.9). Other factors analysed for original choice of health facility as delivery site included concerns about male health workers conducting the delivery. Mothers who were not bothered if their delivery was conducted by male health workers were more likely to opt for facility delivery (POR= 1.1, 95% CI: 1.0 - 1.2). Similarly, women who resided in communities which had sanctions for home delivery were more likely to have the health facility as their original choice of delivery site (POR= 1.1, 95% CI: 1.0 - 1.2).
Table 4. Needing permission was not significantly associated with original choice of delivery site (POR: 0.9, 95% CI: 0.8 - 1.0). Original choice of delivery site was also not associated with mother´s level of education, age, previous delivery experience such as death of babies and number of previous deliveries.
Discussion
In this study, 84% of women in Liberia chose to deliver their babies at the health facility. This is higher than the 56% documented in the LDHS 2013 [5] and 74.5% reported in the Multiple Indicator Cluster survey[10]. This inferred a level of progress has been made with regards to the campaign to increase health facility-based delivery [11]. Maternal death has been identified as a health policy priority in Liberia [12]. Several health interventions were implemented after the Ebola Virus Disease outbreak addressing health-facility delivery amongst other reproductive health interventions [13, 14]. Some of the health interventions were targeted at increasing health facility delivery. Women who had preference for hospital delivery utilized health care facilities while those who saw no benefit mostly had their babies delivered at home. The finding that health-facility delivery was generally regarded as beneficial could be a result of intense public health education that has been conducted since 2015 as part of the national strategy to improve maternal outcomes [11]. Intense public health awareness campaigns have helped to improve health education across different settings. Compared to other developing countries like Uganda, Ethiopia and India [15-17], the proportion of women who chose health-facility delivery was higher. The majority of those who abandoned an original attempt at home delivery eventually had caesarean section at the health facility. This could have resulted in maternal and/or foetal deaths if home delivery was not abandoned.
Knowledge about the benefits of ANC and health-facility delivery was found to be high, even among those who chose home delivery for various reasons. From our study, adequate knowledge and patronage of ANC was positively associated with choice of health facility, like findings in Nigeria and Nepal [
10,
11]. Mothers who were not bothered whether their delivery was conducted by a male or female health worker were more likely to choose health-facility delivery. A higher preference for delivery at health facilities may however not be obtainable among religious women who would not allow their delivery to be handled by males.
A few respondents cited unpleasant language from health workers as a reason for choosing home delivery over health-facility delivery. Since the study did not detail the actual offensive words used by the health workers, this remained within the judgement of the mothers. A study in Ethiopia similarly concluded that positive attitude of health workers promoted facility delivery [
6].
In Liberia, delivery services at public health facilities are supposed to be free per directives from the Ministry of Health, although there are undocumented reports of patients having to pay for some items. Private facilities on the other hand operate cash for service at service delivery points. From the study, lower income earners were found to be more likely to choose facility delivery. The discussion of this finding is limited since the study did not disaggregate private from public health facilities.
Community sanctions against home deliveries increased the number of women utilizing the hospital for delivery. Social and cultural considerations were also noted to determine utilization of health care facilities by pregnant women in a small community in Nigeria [
18]. Maternal education and enlightenment has been shown to improve the utilization of facility-based delivery [
11], however this was not corroborated in our study.
Limitations
Recall bias was a possible limitation. However, we limited most questions to the last childbirth to minimise the bias. Social desirability bias was reduced by ensuring mothers were properly informed about the study and assured their candid opinions would be useful in improving the health status of women in Liberia. The key message was limited by the low number responses in the Home delivery group, however the sample size was increased from 30 by 7 to 30 by 21 to include more mothers. Mothers interviewed were those who had recently delivered. Visitors and non-permanent residents of the community, and non-consenting eligible women were excluded. The exclusion could not have introduced a form of selection bias since the women in such categories were few.
Conclusion
More study participants chose health facilities as the preferred place of delivery in Liberia. The choice of delivery site was influenced by participants´ knowledge of the benefits of health facility delivery. Early and frequent attendance at ANC, and sanctioning of home deliveries within the communities determined the choice of delivery site.
Recommendations
The County Health Teams should continue to sensitize the community on the benefits of delivering at the health facility and encourage improvement in staff attitude and communication towards clients. The involvement of community authorities would increase their commitment to health-facility delivery.
What is known about this topic
- Women make decision to deliver.
- High ratio of maternal mortality in Liberia at 1072/100,000 live birth.
- Poor antenatal care visit and low health facility delivery are common in Liberia.
What this study adds
- More study participants chose health facilities as the preferred place of delivery in Liberia.
- The choice of delivery site was influenced by participants´ knowledge of the benefits of health facility delivery.
- Early and frequent attendance at ANC, and sanctioning of home deliveries within the communities determined the choice of delivery site.
Competing interests
The authors declare no competing interests.
Authors' contributions
Gabriel B. Kassay conceptualized, wrote the draft methodology, carried out supervision, did data entry and cleaning as well as did final corrections from the reviewers, and final manuscript submission. Olayinka Stephen Ilesanmi supported the planning with drafting plan, supervision, formal analysis, final correction from peer reviewers and chief editor. Peter Adewuyi supported the planning, carried out supervision and formal analysis. Maamie Amo-Addae guided the process with technical ideas, carried out supervision, review and editing of manuscript draft and also offered technical and administrative assistance. Wede Himiede Wilson participated in planning, supervision, review and editing of draft manuscript. Obafemi Babalola supervised and reviewed draft manuscript. Ben Gbouh, Dedesco Gweh, Emmanuel Dweh, Emmanuel Ghartey, Feleciai Dweh, Lawrence Larway, Leroy Maximore, Moses Fomba , Sylvester Toe, Tamba Alpha, Faith Whesseh, Roseline George, Trokon Yeabah, participated in data collection, entry and general review.
Acknowledgements
Ministry of Health, Liberia, National Public Health Institute of Liberia (NPHIL), Liberia Field Epidemiology Training Programme, United States Centers for Disease Control and Prevention, African Field Epidemiology Network.
Tables and figures
Table 1: Sociodemographic characteristics of women who gave birth in Liberia, 2017
Table 2: Sociodemographic characteristics and the initial choice of delivery site, Liberia, 2017
Table 3: Reasons initial, final and change in decision with delivery site in Liberia, 2017
Table 4: Factors associated with initial place of attempted delivery, Liberia 2017
Figure 1: Counties of residence and initial choice of delivery site in Liberia, 2017
References
- WHO. Maternal mortality-key facts. WHO. 2019. Accessed May 2020.
- Callister LC, Edwards JE. Sustainable Development Goals and the Ongoing Process of Reducing Maternal Mortality. Journal of Obstetric, Gynecologic & Neonatal Nursing. 2017; 46(3):e56-e64.https://doi.org/10.1016/j.jogn.2016.10.009 . Google Scholar
- Wereta T, Betemariam W, Karim AM, Fesseha Zemichael N, Dagnew S, Wanboru A, et al. Effects of a participatory community quality improvement strategy on improving household and provider health care behaviors and practices: a propensity score analysis. BMC Pregnancy and Childbirth. 2018; 18(Suppl 1):364.https://doi.org/10.1186/s12884-018-1977-9 . PubMed | Google Scholar
- World Health Organization. Strategies toward ending preventable maternal mortality (EPMM). WHO. 2015. Accessed September 2019.
- Liberia Institute of Statistics and Geo-Information Services. Liberia Demographic and Health Survey 2013. Liberia Institute of Statistics and Geo-Information Services, Ministry of Health and Social Welfare, National AIDS Control Program & ICF International. 2013. Accessed September 2019.
- Population pyramid.net. Liberia 2017. Population pyramid.net .2019. Accessed October 2019.
- UNFPA Liberia. Sexual and Reproductive Health. UNFPA Liberia. 2018. Accessed October 2018.
- IBM SPSS Statistics for Windows. Version 21.0. IBM Corp. Released 2012. Armonk, NY: IBM Corp.
- CDC. EPI INFO 7 2008.CDC. 2015. Accessed September 2015.
- United Nations Children´s Fund (UNICEF). Liberia Multiple Indicator Cluster Survey. 2016.
- Yaya S, Uthman OA, Bishwajit G, Ekholuenetale M. Maternal health care service utilization in post-war Liberia: analysis of nationally representative cross-sectional household surveys. BMC Public Health. 2019; 19:28.https://doi.org/10.1186/s12889-018-6365-x . PubMed | Google Scholar
- Lalthapersad-Pillay P. Joyce Banda and Ellen Johnson Sirleaf - confronting the neglect of maternal health and women´s rights in Malawi and Liberia. Agenda. 2019; 33(1):97-107.https://doi.org/10.1080/10130950.2019.1605679 . Google Scholar
- The World Bank. World Bank Approves $16 Million to Support Reproductive, Maternal and Child Health in Liberia. World Bank. 2017. Accessed October 2019.
- USAID. Improving maternal and child health is key to furthering Liberia´s development. USAID. 2015. Accessed October 2018.
- Belay A, Sendo E. Factors determining choice of delivery place among women of child bearing age in Dega Damot District, North West of Ethiopia: a community based cross- sectional study. BMC Pregnancy and Childbirth. 2016; 16:229.https://doi.org/10.1186/s12884-016-1020-y . PubMed | Google Scholar
- Agnes A, David M, George B, Fred N. Predictors for health-facility delivery in Busia district of Uganda: a cross sectional study. BMC Pregnancy Childbirth. 2012; 12:132.https://doi.org/10.1186/1471-2393-12-132 . PubMed | Google Scholar
- Nair M, Ariana P, Webster P. What influences the decision to undergo institutional delivery by skilled birth attendants? A cohort study in rural Andhra Pradesh, India. Rural Remote Health. 2012; 12:4. Google Scholar
- Brieger WR, Luchok KJ, Eng E, Earp JA. Use of maternity services by pregnant women in a small Nigerian community. Health Care Women Int. 1994; 15(2):101-10.https://doi.org/10.1080/07399339409516102 . PubMed | Google Scholar